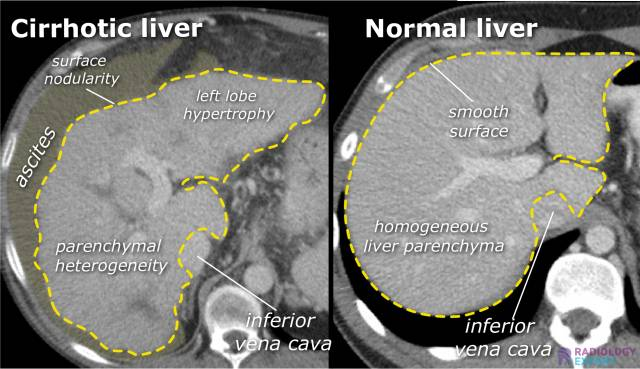
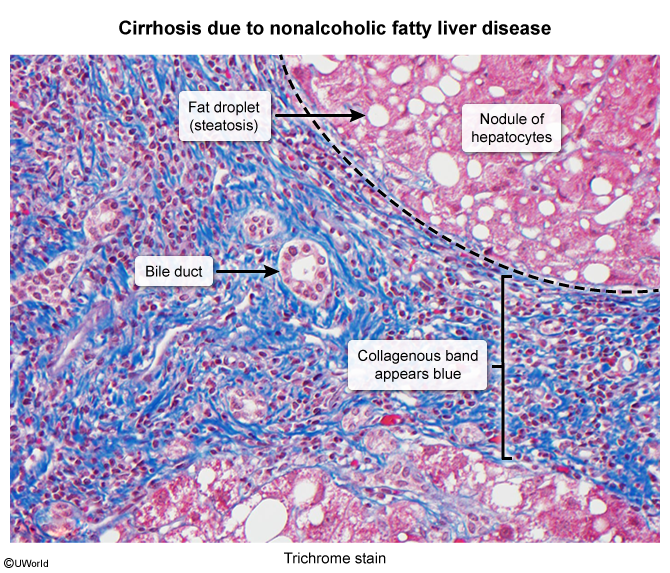
Replacement of normal liver tissue with collagenous regenerative nodules
Treatment
Complications
Portal hypertension
Portal-Caval Anastomoses
These are connections between the portal venous system and the systemic (caval) venous system. In portal hypertension, these sites become engorged and dilated as blood is shunted away from the high-pressure liver.
Esophageal:
Portal: Left Gastric Vein
Caval: Esophageal branches of the Azygos Vein (drains to SVC)
Clinical:Esophageal Varices (risk of life-threatening hematemesis).
Urgent EGD: For banding/ligation of bleeding varices.
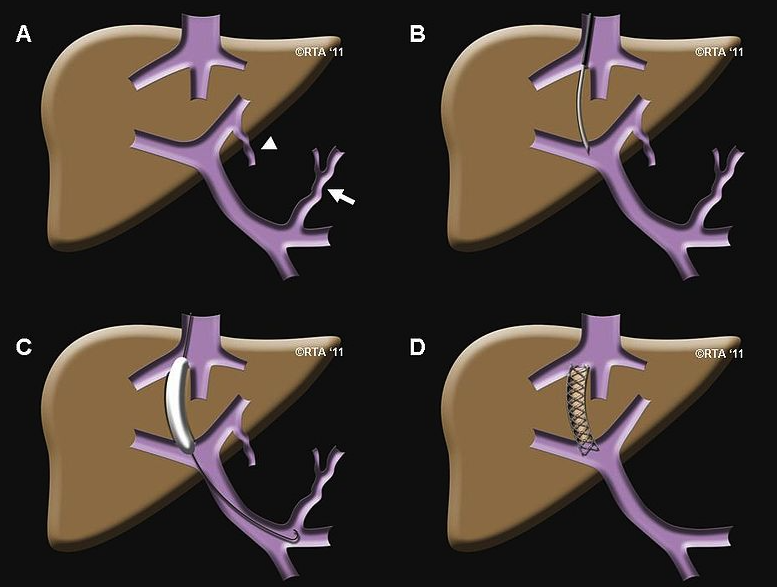
Refractory Bleeding/Ascites:
Transjugular Intrahepatic Portosystemic Shunt (TIPS): A stent placed between the portal vein and hepatic vein, shunting blood to decompress the portal system. Risk of worsening hepatic encephalopathy.
Ascites Management: Sodium restriction, diuretics (spironolactone, furosemide), and paracentesis for large volumes.
Definitive Treatment: Liver transplantation for end-stage liver disease.
Pulmonary complications of cirrhosis
Hepatic hydrothorax
Definition: pleural effusions (typically one-sided; 70% right, 18% left) with transudate characteristics in the absence of any other cardiac, pulmonary, or pleural disease
Pathophysiology: increased permeability of the diaphragm (small defects, increased abdominal pressure)