- Epidemiology
- Most common in individuals 50–70 years of age
- Etiology & Risk Factors
- Offending Agents (Classic “SHIPP-E” Mnemonic):
- Sulfa drugs
- Hydralazine
- Isoniazid (INH)
- Procainamide (Highest risk)
- Phenytoin
- Etanercept (and other TNF-α inhibitors)
- Others: Minocycline, Quinidine, Methyldopa.
- Risk Factors: Slow acetylators (Phase II metabolism, hepatic N-acetyltransferase deficiency) are at ↑ risk due to accumulation of drug metabolites.
- Offending Agents (Classic “SHIPP-E” Mnemonic):
- Pathophysiology
- Drugs or their metabolites bind to proteins/DNA, creating neoantigens that stimulate an autoimmune response.
- Often involves genetic susceptibility (e.g., HLA-DR4).
- Clinical features (usually manifest ≥ 1 month after medication initiation)
- Constitutional: fatigue, fever, and weight loss
- Musculoskeletal: myalgia and symmetrical polyarthralgia
- Skin lesions (e.g., malar rash)
- Diagnostics
- ANAs are positive in nearly all patients.
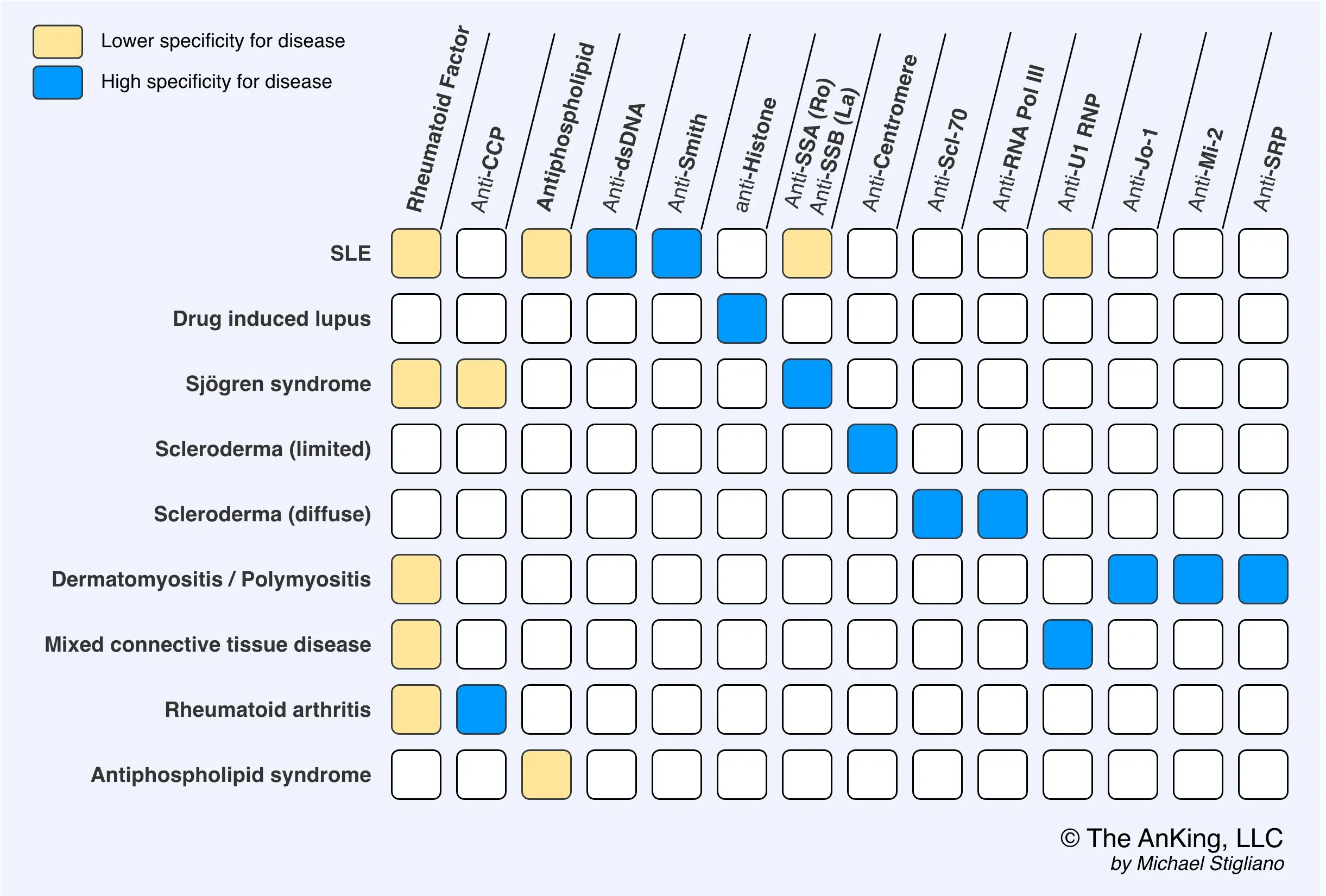
- Antihistone antibodies
- Antihistone antibodies are seen in 90–95% of patients.
- Antihistone antibodies are seen in 90–95% of patients.
Tip