- Patho/Etiology
- Caused by Vitamin B12 (cobalamin) deficiency, which leads to defective myelin synthesis and maintenance.
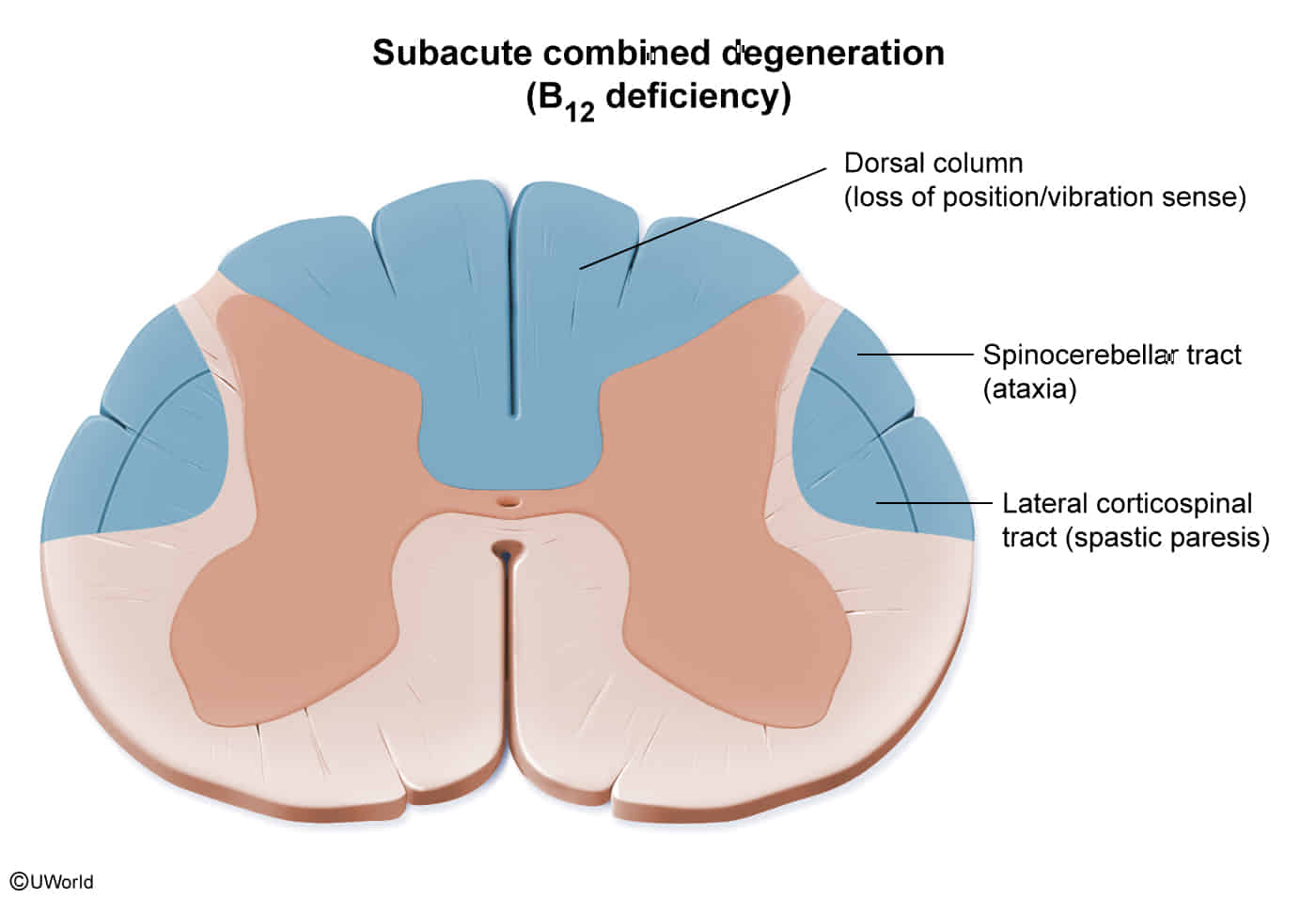
- The name “combined” refers to the degeneration of multiple spinal cord tracts.
- Affected Tracts:
- Dorsal Columns: Loss of vibration sense, proprioception, and fine touch.
- Lateral Corticospinal Tracts: Spastic paresis, hyperreflexia, and a positive Babinski sign.
- Spinocerebellar Tracts: Ataxia.
Tip
Affects heavily myelinated tracks (proprioception, motor) but not light/no myelinated tracks (pain, temp) t
- Causes of B12 Deficiency
- Pernicious Anemia: Autoimmune destruction of gastric parietal cells, leading to a lack of intrinsic factor. This is the most common cause.
- Malabsorption: Conditions like Crohn’s disease, celiac disease, or prior gastrectomy/ileal resection.
- Dietary Insufficiency: Rare, but can be seen in strict vegans over many years.
- Other: Diphyllobothrium latum (fish tapeworm) infestation, chronic nitrous oxide abuse.
- Clinical Presentation
- Symmetric and progressive.
- Sensory: Begins with distal, symmetric paresthesias (numbness, tingling) in the feet and hands. Loss of vibration and position sense is often the first sign.
- Motor: Spastic weakness, especially in the lower limbs. An initially flaccid paralysis can become spastic over time.
- Gait: Ataxic gait due to combined sensory and cerebellar tract dysfunction.
- Reflexes: May show a combination of UMN signs (hyperreflexia, Babinski) from corticospinal tract damage and LMN signs (absent Achilles reflex) from a concurrent peripheral neuropathy.
- Neuropsychiatric: Irritability, apathy, “megaloblastic madness” (paranoia, delirium), and cognitive impairment can occur.
- Diagnosis
- Labs:
- Low serum Vitamin B12 level.
- Elevated serum methylmalonic acid (MMA) and homocysteine levels. These are more sensitive than B12 levels alone.
- CBC: May show a megaloblastic anemia (↑ MCV) with hypersegmented neutrophils, but neurologic symptoms can occur without anemia.
- Antibodies against intrinsic factor or parietal cells if pernicious anemia is suspected.
- Imaging:
- MRI of the spinal cord is not usually required for diagnosis but can show T2-weighted hyperintensities in the dorsal columns of the cervical and thoracic spine.
- Labs:
- Management
- Immediate B12 supplementation is crucial to prevent irreversible neurological damage.
- Tx: Intramuscular (IM) or subcutaneous injections of vitamin B12 are standard, especially when neurologic symptoms are present.
- A typical regimen starts with daily or alternate-day injections for 1-2 weeks, followed by weekly, then monthly injections for life (if the underlying cause is irreversible).
- Prognosis: Early treatment (within weeks) can lead to a complete recovery; however, long-standing deficits are often permanent.
- Caution: Never treat megaloblastic anemia with folic acid alone without first ruling out B12 deficiency. Doing so will correct the anemia but will not stop the progression of the potentially irreversible neurologic damage of SCD.