Etiology
Classifications
Tip
Squamous and small cell carcinomas are sentral (central) and often caused by tobacco smoking.
Non-small cell lung cancer (NSCLC)
Adenocarcinoma
- Location: Peripheral
- Characteristics
- Most common type of primary lung cancer
- More common in women and nonsmokers
- Associated with mutations in:
- EGFR gene
- ALK gene
- KRAS gene
- Common finding: hypertrophic osteoarthropathy (digital clubbing)
- Most common type of lung cancer that originates in pulmonary scars
- Prognosis is usually better than in other types of lung cancer
Adenocarcinoma of Lung Kinase”: Cancer (adenocarcinoma of lung) and the gene product (tyrosine kinase) are associated with ALK mutations.
“
Large cell carcinoma
- Location: Peripheral
- Characteristics
- Strong association with smoking
- Poor response to chemotherapy
- Early metastases
- Poor prognosis
Squamous Cell Carcinoma
- Location: Central (Hilar mass arising from bronchus).
- Histology: Keratin pearls, intercellular bridges (desmosomes).
- Associations: Strong smoking history.
- Complications: Cavitation, Hypercalcemia (produces PTHrP).
Lung neuroendocrine tumors
Histology
- Neuroendocrine Kulchitsky cells
- Rapid growth pattern
- Expressed tumor markers
- Chromogranin A
- Synaptophysin
- Neuron-specific enolase
Small cell lung cancer (SCLC)
- Location: Peripheral
- Characteristics
- Strong association with smoking
Bronchial carcinoid tumor
- Location: Central or peripheral
- A rare type of neuroendocrine lung tumor that consists predominantly of neuroendocrine Kulchitsky cells
- Characteristics
- Most common primary lung tumor in children/adolescents.
- Typical age: Young adults (20-40 y/o).
- Endobronchial growth leads to airway obstruction:
- Most common primary lung tumor in children/adolescents.
- Neuroendocrine Kulchitsky cells
- Rapid growth pattern
- Expressed tumor markers
- Chromogranin A
- Synaptophysin
- Neuron-specific enolase

Variants of lung cancer
Pancoast tumor
- An apical lung carcinoma
- Located in the superior sulcus of the lung (superior sulcus tumor)
- Predominantly NSCLC
- May lead to the development of Pancoast syndrome
- Cervical sympathetic ganglion (stellate ganglion): Horner syndrome (ipsilateral miosis, ptosis, and anhidrosis)
- Brachial plexus
- Localized pain in the axilla and shoulder (plexus neuralgia)
- Upper limb motor and sensory deficits (e.g., hand muscle weakness and atrophy)
- Recurrent laryngeal nerve: hoarseness
- Brachiocephalic vein
- Unilateral edema of the arm
- Facial swelling
- Phrenic nerve: paralysis of the hemidiaphragm (visible as elevated hemidiaphragm on chest x-ray)
Pathophysiology
Clinical features
Paraneoplastic syndromes
Shared paraneoplastic features and syndromes
NSCLC
Squamous cell carcinoma
- Hypercalcemia of malignancy (increased risk with squamous cell carcinoma)
- Secrete PTHrP
Adenocarcinoma
- Hypertrophic osteoarthropathy
- Clubbing of the fingers and toes (Hippocratic fingers)
- Dermatomyositis or polymyositis
- Migratory thrombophlebitis (Trousseau syndrome)
SCLC (Secretion caused problems, except for PTHrP)
- Cushing syndrome
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
- Lambert-Eaton syndrome, see Myasthenia gravis > Lambert-Eaton myasthenic syndrome (LEMS)
- Cerebellar ataxia
Diagnostics
Microscopic
Adenocarcinoma
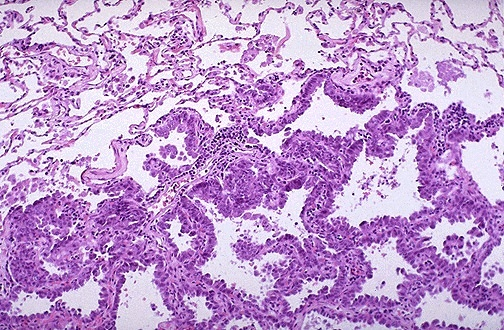 composed of columnar cells that proliferate along the framework of alveolar septae, a so-called “lepidic” growth pattern.
composed of columnar cells that proliferate along the framework of alveolar septae, a so-called “lepidic” growth pattern.
Squamous cell carcinoma
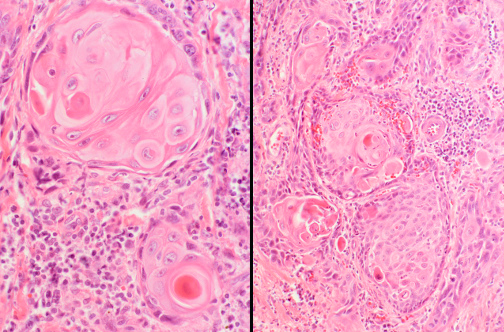
- pink cytoplasm
- keratin pearls
- distinct cell border
Large cell carcinoma
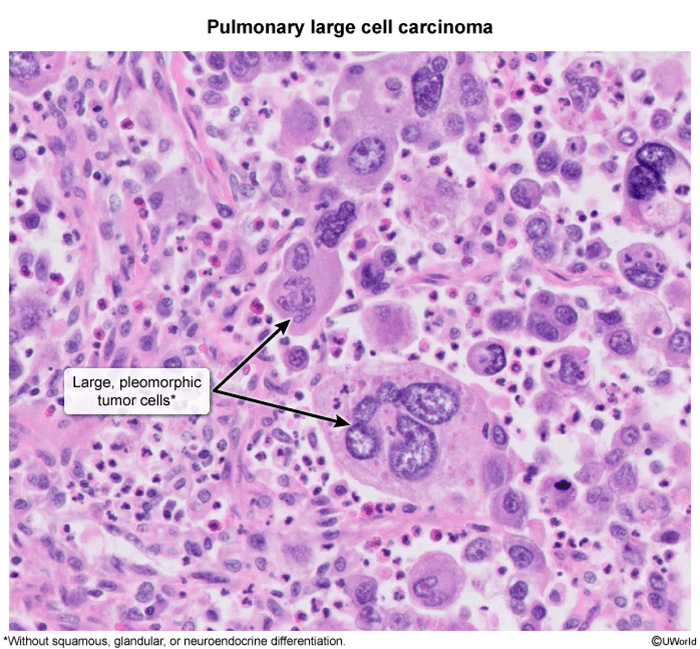
- Undifferentiated
- Large tumor cells
Small cell carcinoma

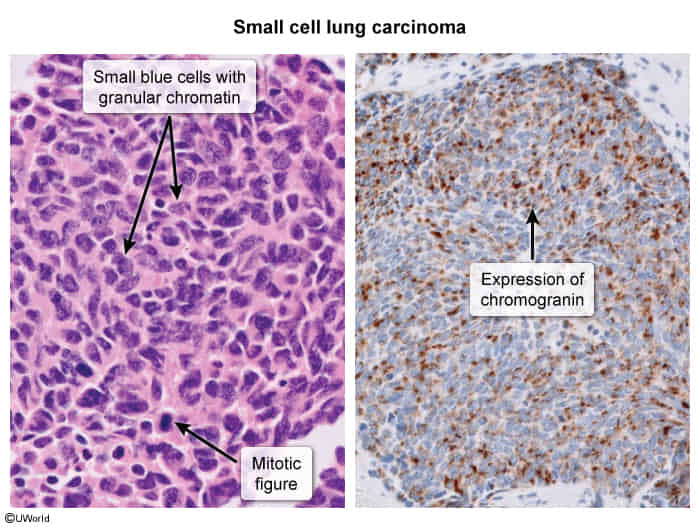 This is the microscopic pattern of a small cell anaplastic (oat cell) carcinoma in which small dark blue cells with minimal cytoplasm are packed together in sheets.
This is the microscopic pattern of a small cell anaplastic (oat cell) carcinoma in which small dark blue cells with minimal cytoplasm are packed together in sheets.
Hamartoma
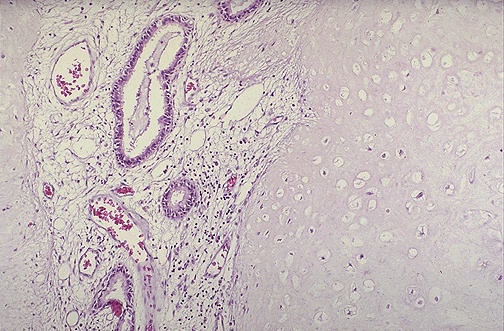 composed mostly of benign cartilage on the right that is jumbled with a fibrovascular stroma and scattered bronchial glands on the left. A hamartoma is a neoplasm in an organ that is composed of tissue elements normally found at that site, but growing in a haphazard mass.
composed mostly of benign cartilage on the right that is jumbled with a fibrovascular stroma and scattered bronchial glands on the left. A hamartoma is a neoplasm in an organ that is composed of tissue elements normally found at that site, but growing in a haphazard mass.
Treatment
Solitary pulmonary nodules
- Epidemiology & Risk Factors
- Definition: Single, well-circumscribed lesion 3 cm, completely surrounded by lung parenchyma, without associated adenopathy, atelectasis, or pleural effusion. (If > 3 cm = lung mass high malignant potential).
- Malignancy Risk Factors:
- Patient: Age 50, active/former smoker, personal Hx of malignancy, occupational exposures (asbestos, radon).
- Nodule: Size 0.8 cm, upper lobe location, spiculated/irregular margins, lack of calcification or eccentric/stippled calcification.
- Diagnosis
- Initial Step: Compare with prior CXR or CT.
- If stable for 2 years benign; no further workup required. c
- If no prior imaging or nodule has grown perform contrast-enhanced Chest CT.
- Risk Stratification & Next Best Steps:
- Low Risk (< 5% malignant probability; < 0.8 cm, young, non-smoker, smooth margins):
- Size < 0.6 cm: No routine follow-up (high-risk patients may need CT in 12 months).
- Size 0.6–0.8 cm: Repeat CT in 6–12 months.
- Intermediate Risk (5–65% probability; 0.8–2.0 cm, mixed features, moderate smoker):
- PET scan or Biopsy (Transthoracic Needle Aspiration [TTNA] for peripheral nodules; Bronchoscopy [FOB] for central nodules).
- If PET (+) or biopsy suggests malignancy surgical resection.
- High Risk (> 65% probability; > 2.0 cm, older, heavy smoker, spiculated, upper lobe): c
- Surgical Resection (Video-Assisted Thoracoscopic Surgery [VATS] or lobectomy) without preceding biopsy.
- Low Risk (< 5% malignant probability; < 0.8 cm, young, non-smoker, smooth margins):
- Benign Calcification Patterns on CT: Diffuse, central, concentric (laminated), or “popcorn” calcifications.
- Initial Step: Compare with prior CXR or CT.
- Management
- Low Risk: Serial surveillance Chest CTs (intervals depend on nodule size/patient risk).
- Intermediate Risk: PET scan to assess metabolic activity if (+), proceed to biopsy or VATS.
- High Risk / Proven Malignancy: VATS resection.