Epidemiology
Leading cause of acute liver failure
Etiology
Pathophysiology
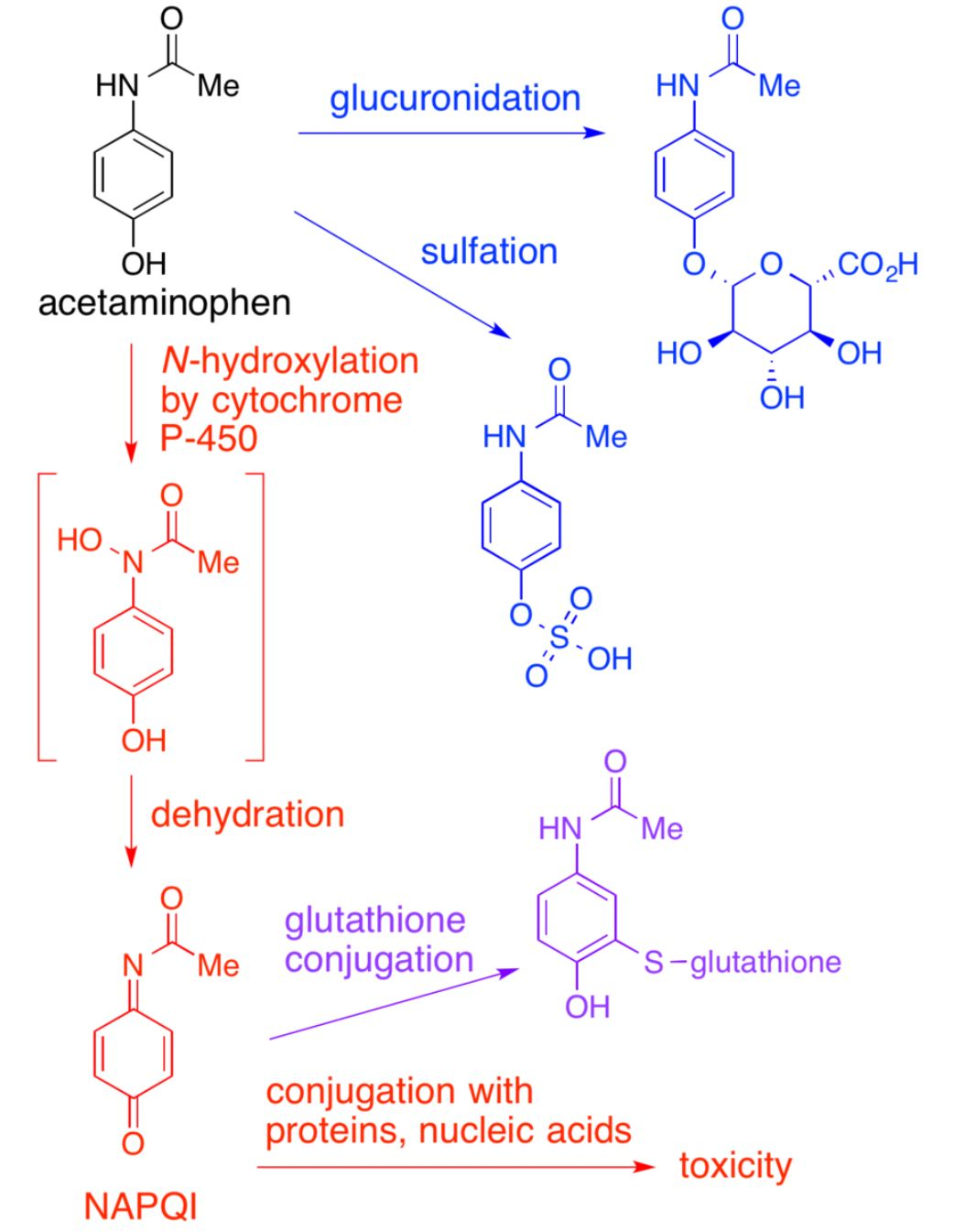
- Exhaustion of hepatic metabolic pathways causes accumulation of a toxic metabolite of acetaminophen, N-acetyl-p-benzoquinoneimine (NAPQI).
- Glutathione initially inactivates NAPQI, but its reserves are eventually depleted, leading to NAPQI accumulation.
- NAPQI → irreversible oxidative hepatocyte injury → liver cell necrosis
- APAP-induced hepatotoxicity
- Defined as peak AST or ALT > 1000 IU/L
- Most commonly caused by APAP overdose
- Occurs rarely at therapeutic doses in patients with:
- Alcohol consumption
- Prolonged fasting
- Chronic liver disease
Clinical features
- Phase 1 (0–24 hours):
- Minimal or non-specific symptoms: Nausea, vomiting, anorexia, diaphoresis, pallor.
- Phase 2 (24–72 hours):
- “Latent period” where systemic symptoms improve, but subclinical hepatotoxicity begins.
- Right upper quadrant (RUQ pain) and tenderness.
- Rising LFTs (AST, ALT, bilirubin) and PT/INR.
- Phase 3 (72–96 hours):
- Peak hepatotoxicity.
- Jaundice, coagulopathy (bleeding/bruising), hepatic encephalopathy (confusion, asterixis).
- Severe cases develop metabolic acidosis, renal failure, and multi-organ dysfunction syndrome (MODS).
- Phase 4 (4 days to 3 weeks):
- Resolution of liver injury (for survivors) or progression to death from liver failure.
Diagnostics
- Initial Test: Serum APAP level drawn at exactly 4 hours post-ingestion (levels drawn <4 hours are uninterpretable due to ongoing absorption).
- Confirmatory/Risk Stratification: Plot the 4-hour (or later up to 24 hours) level on the Rumack-Matthew Nomogram.
- Only valid for a single, acute, immediate-release ingestion.
- If the level lies on or above the treatment line (150 mcg/mL at 4 hours), initiate antidote therapy.
- Key Labs:
- LFTs: AST/ALT > 10,000 U/L in severe toxicity (highest of any toxic/infectious cause). c
- Coagulation studies: PT/INR (most sensitive indicator of liver synthetic function decline).
- BMP: Creatinine (evaluates for acute kidney injury/hepatorenal syndrome), HCO3- (evaluates for metabolic acidosis).
- Arterial Blood Gas (ABG): pH and lactate (essential for prognosticating liver transplant need).
Differential diagnostics
| Feature | Salicylate (ASA) | Acetaminophen (APAP) | Reye Syndrome |
|---|---|---|---|
| Path | Uncouple oxidative phosphorylation (leads to hyperthermia); Direct stimulation of resp center. | Glutathione depletion NAPQI centrilobular hepatic necrosis. | Mito dysfunction ( -oxidation) Microvesicular fatty change in liver |
| Hx/Trigger | OD; Wintergreen oil | OD (esp. w/ CYP inducers/EtOH) | Child + Virus + ASA |
| Key Sx | Tinnitus, Hyperthermia, Tachypnea | RUQ pain, Fulminant liver failure | Encephalopathy, Vomiting |
| Labs/Path | Mixed Resp Alk + Met Acidosis | Zone 3 Necrosis, AST/ALT | Microvesicular fatty liver, Glucose, Ammonia |
| Tx | NaHCO3 (Alkalinize urine), Dialysis | N-acetylcysteine (restore glutathione) | Supportive |
Treatment
- Airway, Breathing, Circulation (ABCs): Establish IV access and stabilize.
- Activated Charcoal: Administer if patient presents within 4 hours of ingestion and is awake/cooperative with a protected airway.
- N-acetylcysteine (NAC):
- Restores glutathione reserves to safely detoxify the toxic metabolite NAPQI.
- Indicated if:
- APAP level is above the treatment line on the Rumack-Matthew Nomogram.
- Ingestion history >150 mg/kg (or >7.5 g total) and lab results are not immediately available.
- Unknown ingestion time + detectable APAP level or elevated transaminases.
- Late presentation (>8–24 hours post-ingestion) with suspected overdose.
- Consensus stopping criteria (do not stop NAC until all are met):
- APAP level <10 mcg/mL.
- INR <2.0.
- AST/ALT are normal or significantly decreased (by 25–50% from peak).
- Patient is clinically well.
- Refractory/Definitive (Liver Transplantation): c
- Evaluated using King’s College Criteria for APAP toxicity:
- Arterial pH <7.3 after fluid resuscitation, OR
- All three of the following: INR >6.5, Creatinine >3.4 mg/dL, and Grade III/IV hepatic encephalopathy.
- Evaluated using King’s College Criteria for APAP toxicity: