FIB-4 > 2.67: High risk of advanced fibrosis; warrants direct hepatology referral.
Secondary Non-Invasive Testing (if FIB-4 is indeterminate):
Vibration-Controlled Transient Elastography (VCTE / FibroScan) or MRE to measure liver stiffness.
Confirmatory/Gold Standard:
Liver Biopsy: Indicated if diagnosis is uncertain, to rule out co-existing etiologies, or to stage fibrosis.
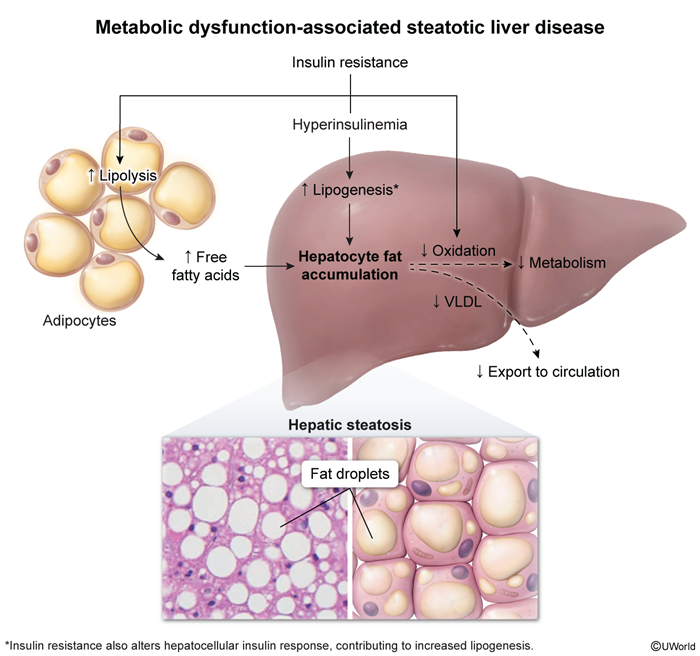
Histology reveals macrovesicular steatosis (>5% of hepatocytes), lobular inflammation, hepatocyte ballooning, and Mallory-Denk bodies.
Key Labs:
Mild elevation of ALT and AST (ALT typically > AST; a reversal to AST > ALT suggests progression to cirrhosis).
Mild elevation of ALP.
Exclude other causes: negative viral hepatitis serologies (HBV, HCV), normal iron studies (ferritin, transferrin saturation), normal ceruloplasmin, and negative ANA/ASMA.
Differential Diagnostics
Alcohol-Associated Liver Disease (ALD):
Differentiating feature: History of significant alcohol intake (>140g/week for females, >210g/week for males). AST:ALT ratio is typically >2:1.
Medication-Induced Steatosis:
Differentiating feature: History of exposure to steatogenic agents (e.g., amiodarone, methotrexate, valproate, tamoxifen, systemic corticosteroids).
Autoimmune Hepatitis (AIH):
Differentiating feature: Elevated serum IgG levels, positive ANA and ASMA, and interface hepatitis on biopsy.
Hereditary Hemochromatosis:
Differentiating feature: Elevated transferrin saturation (>45%), high ferritin, and HFE gene mutation.
Wilson Disease:
Differentiating feature: Younger age of onset (<35 years), decreased ceruloplasmin, Kayser-Fleischer rings, and neuropsychiatric symptoms.
Management
First-line (Lifestyle Interventions):
Weight loss: Target ≥7-10% of total body weight (promotes resolution of steatohepatitis and regression of fibrosis).
Dietary modification: Mediterranean diet (low carbohydrates, high monounsaturated fats), strict avoidance of fructose and sweetened beverages.
Exercise: 150 minutes/week of moderate-intensity aerobic and resistance training.
Aggressive management of CV risk factors (statin therapy for dyslipidemia, tight glycemic control, BP control).
Second-line (Pharmacotherapy):
For patients with concurrent DM2: GLP-1 receptor agonists (e.g., semaglutide) or Pioglitazone.
For non-cirrhotic MASH with moderate-to-advanced fibrosis (stages F2-F3): Resmetirom (thyroid hormone receptor-beta selective agonist).
Vitamin E (800 IU/day): Considered for non-diabetic patients with biopsy-proven MASH.
Refractory / Advanced Disease:
Bariatric surgery: Recommended for eligible patients (BMI ≥35 kg/m²) with refractory MASLD/MASH to achieve sustained weight loss.
Liver transplantation: Indicated for decompensated MASH-related cirrhosis or MASH-associated HCC.
Complications
Progression to Metabolic Dysfunction-Associated Steatohepatitis (MASH).
Liver Cirrhosis and portal HTN.
Hepatocellular Carcinoma (HCC): Can develop in patients with MASLD/MASH even in the absence of cirrhosis.
Cardiovascular Disease (CVD): The leading cause of mortality in patients with MASLD/MASH.