Epidemiology
Etiology
Pathophysiology
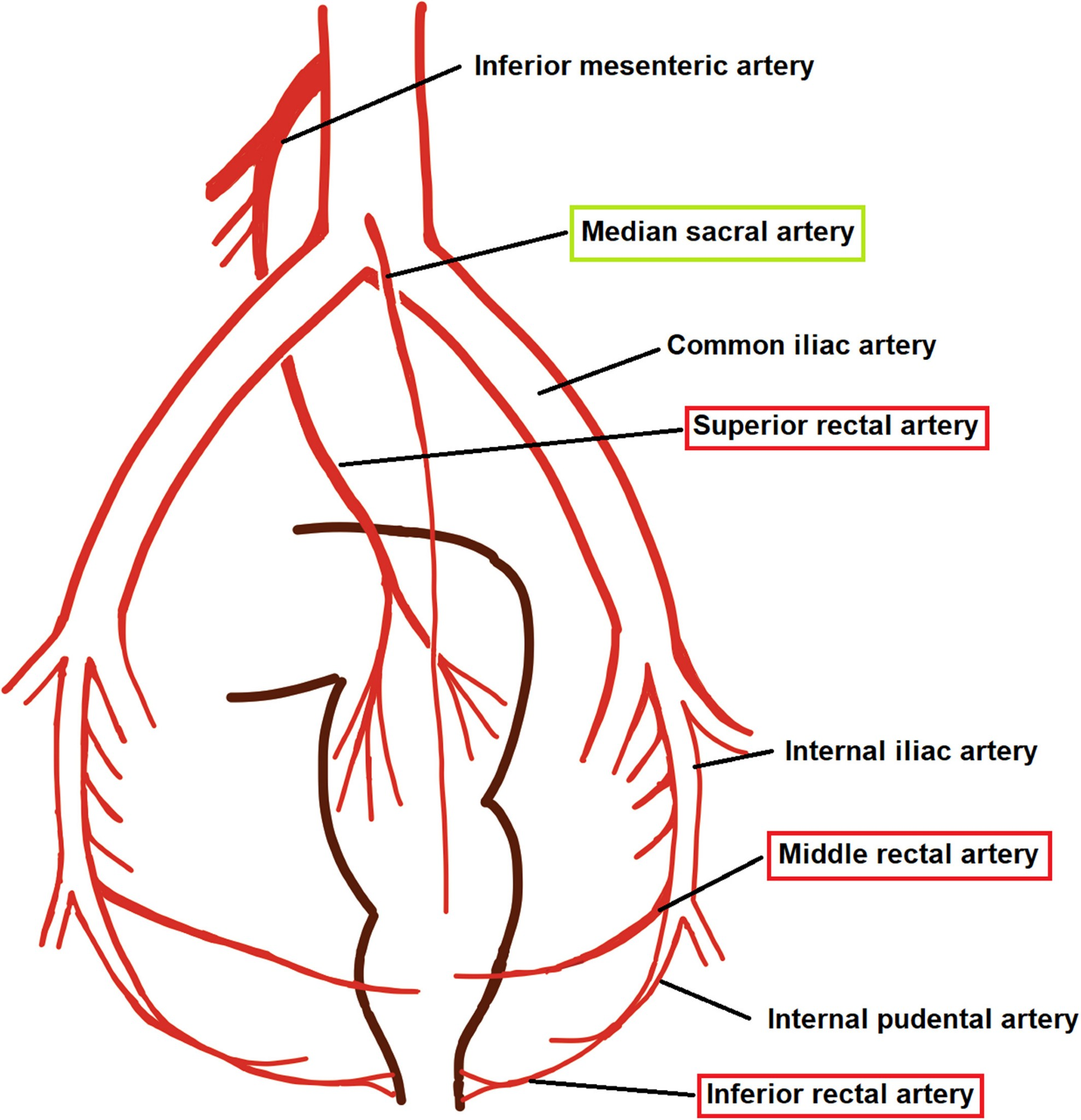
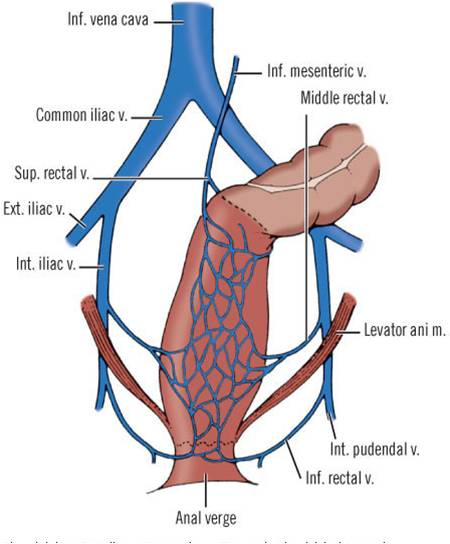
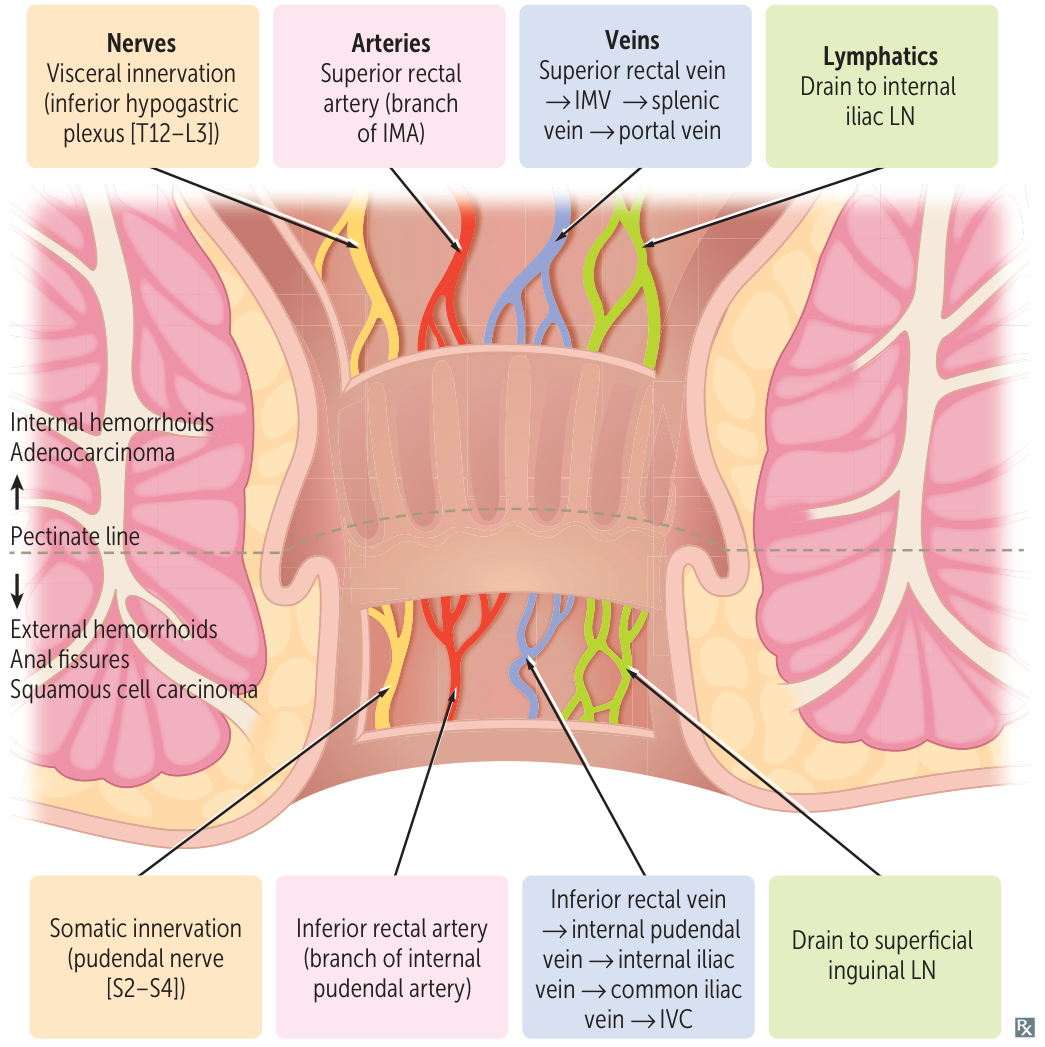
Anatomy of the anal canal
Tip
- Think the rectum above the pectinate line is still part of GI tract, so it’s all related to GI (inferior mesenteric artery/vein, inferior hypogastric plexus)
- Think the rectum below the pectinate line is part of genitalia, so it’s all related to pudendum (internal pudendal artery/vein, pudendal nerve)
Clinical features
Diagnostics
Treatment
- Conservative (First-line for Grade I-II internal, non-thrombosed external):
- High-fiber diet (25-35g/day), increased oral fluid intake, and avoidance of straining.
- Sitz baths (warm water helps relax the internal anal sphincter and soothe the area).
- Topical anesthetics (e.g., pramoxine, lidocaine) or topical corticosteroids (e.g., hydrocortisone; limit to <2 weeks to avoid mucosal/skin atrophy).
- Office-Based Interventions (Second-line for Grades I-III internal failing medical therapy):
- Rubber band ligation (most common and effective; causes ischemic necrosis and subsequent scarring of the hemorrhoid).
- Contraindications: Immunocompromised patients, patients on systemic anticoagulation (due to risk of delayed, severe arterial bleeding).
- Infrared coagulation or sclerotherapy (alternatives for low-grade internal hemorrhoids).
- Rubber band ligation (most common and effective; causes ischemic necrosis and subsequent scarring of the hemorrhoid).
- Surgical Interventions (Third-line):
- Surgical Hemorrhoidectomy: Indicated for Grade IV internal hemorrhoids, mixed internal/external hemorrhoids, or failure of office-based procedures.
- Acutely Thrombosed External Hemorrhoids:
- Onset <72 hours: Excision of the thrombus/hemorrhoid under local anesthesia (provides immediate pain relief). c
- Onset >72 hours: Conservative management (symptomatic treatment with sitz baths, analgesics, and stool softeners, as the pain has already peaked and the clot will gradually resorb).