Epidemiology
Frequency: hepatic hemangioma (most common) > focal nodular hyperplasia (FNH) > hepatocellular adenoma (rare)
Etiology
- Hepatic Hemangioma: Most common benign liver lesion. F > M (usually age 30–50). Associated with pregnancy, estrogen use, and OCP use (can enlarge).
- Focal Nodular Hyperplasia (FNH): Second most common benign liver lesion. Primarily in young females (F > M). Not strictly OCP-dependent (though can grow under hormonal influence).
- Hepatic Adenoma: Strongly associated with OCP use and anabolic steroids. Also associated with glycogen storage diseases (e.g., Von Gierke). Young females (F >> M). c
- Hepatocellular Carcinoma (HCC): Most common primary hepatic malignancy. Associated with cirrhosis (secondary to HCV, HBV, alcoholism, NASH), hemochromatosis, and aflatoxin B1 exposure.
- Metastatic Disease: Most common liver malignancy overall. Usually secondary to primary malignancies of the colon, pancreas, lung, breast, or stomach.
Hepatic Adenoma
Epidemiology & Risk Factors
- Predominantly young females (20-40yo).
- Strong association with oral contraceptive pills (OCPs) (dose and duration-dependent).
- Other risk factors:
- Anabolic steroid use.
- Glycogen storage diseases (type I and III).
- Obesity and metabolic syndrome.
Clinical Features
- Asymptomatic: Often found incidentally on imaging.
- Symptomatic: Right upper quadrant (RUQ) pain or fullness due to mass effect or minor intratumoral hemorrhage.
- Acute Rupture: Sudden-onset, severe RUQ pain, radiating to the right shoulder, signs of peritonitis, and hemorrhagic shock (hypotension, tachycardia) due to hemoperitoneum. c
Diagnosis
- Initial Imaging: RUQ US (non-specific, well-demarcated echogenic mass).
- Confirmatory/Gold Standard Imaging: Contrast-enhanced MRI of the liver (preferred over CT). Shows arterial enhancement with variable washout.
- Key Labs:
- AFP is normal (crucial to differentiate from HCC).
- LFTs and liver function are typically normal.
- Biopsy: Generally contraindicated due to high risk of bleeding/rupture and sampling error.
Management
- Discontinue OCPs (or offending steroids/medications) in all patients.
- Asymptomatic & Small (< 5 cm):
- Conservative management.
- Stop OCPs + serial imaging (MRI/US) every 6-12 months.
- Symptomatic, Large (≥ 5 cm), or Male patients:
- Surgical resection (high risk of rupture and malignant transformation, especially in males).
- Pregnancy planning:
- Resection recommended for tumors ≥ 5 cm prior to pregnancy due to high estrogen-induced risk of rupture during gestation.
- Ruptured/Unstable patient:
- Hemodynamic resuscitation + urgent transcatheter arterial embolization (TAE) followed by elective resection of remaining tumor once stable.
Complications
- Rupture & Hemorrhage: High risk during pregnancy (estrogen stimulates tumor growth) and if tumor is > 5 cm.
- Malignant Transformation: Risk of progression to HCC (especially in males, β-catenin mutated subtypes, or large tumors).
Diagnostics
- Ultrasonography: best initial test
- Biopsy
- Performed to confirm the diagnosis if imaging is inconclusive
- Contraindicated in hepatic hemangiomas, as it may cause bleeding
- Pathology
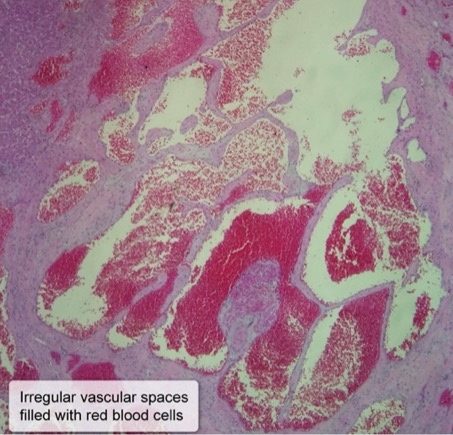
- Hepatic hemangioma
- Cavernous vascular spaces of variable size, lined by flat endothelial cells
- Cavernous vascular spaces of variable size, lined by flat endothelial cells
- Hepatic hemangioma