Psoas sign: RLQ pain with passive extension of right hip (indicates retrocecal appendix). c
Obturator sign: RLQ pain with passive internal rotation of flexed right hip (indicates pelvic appendix).
McBurney point tenderness: Maximal tenderness 1/3 of the distance from the ASIS to the umbilicus.
Diagnostics
Primarily a clinical diagnosis; typical presentations in males do not require imaging before surgery.
Labs: ↑ WBC (leukocytosis with left shift). Beta-hCG in all females of childbearing age to rule out ectopic pregnancy.
Imaging (if Dx unclear):
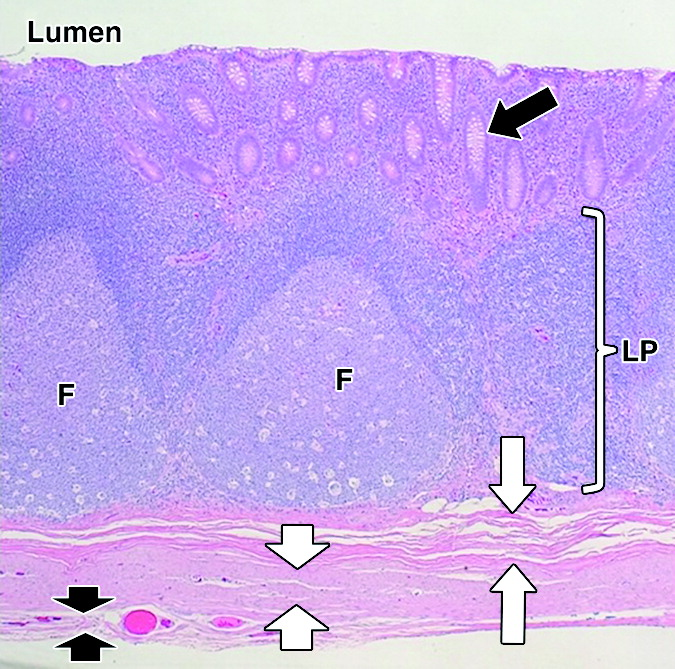
CT abdomen/pelvis with contrast (preferred in adults): Shows thickened wall (>6 mm), target sign, appendiceal wall enhancement, and periappendiceal fat stranding.
Ultrasound or MRI (preferred in pregnant pts and children to avoid radiation).
Treatment
Special patient groups
Appendicitis in pregnant individuals
Clinical Features
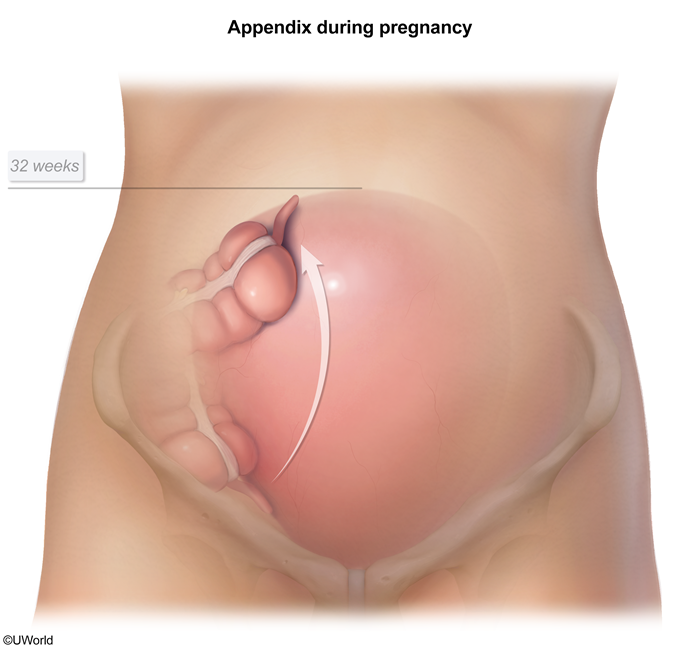
Anatomical displacement: The growing gravid uterus displaces the appendix upward and outward (counterclockwise rotation).
Atypical pain location:
RLQ pain in the 1st trimester (similar to non-pregnant).
RUQ or right flank pain in the 3rd trimester as the appendix is displaced superiorly.
Nausea and vomiting: Present in majority of cases, but frequently dismissed as normal pregnancy-related symptoms (e.g., morning sickness).
Peritoneal signs: Guarding and rebound tenderness are often absent or diminished because the gravid uterus lifts the abdominal wall away from the inflamed appendix.
Alder sign: Pain does not shift when the pt is turned onto the left lateral decubitus position, pointing to an extrauterine etiology.