A genetic disorder that is characterized by decreased urinary calcium excretion and (usually asymptomatic) hypercalcemia. PTH levels are normal in most patients. Caused by an autosomal dominant mutation of a calcium-sensing receptor in the kidneys and parathyroid gland (CaSR gene).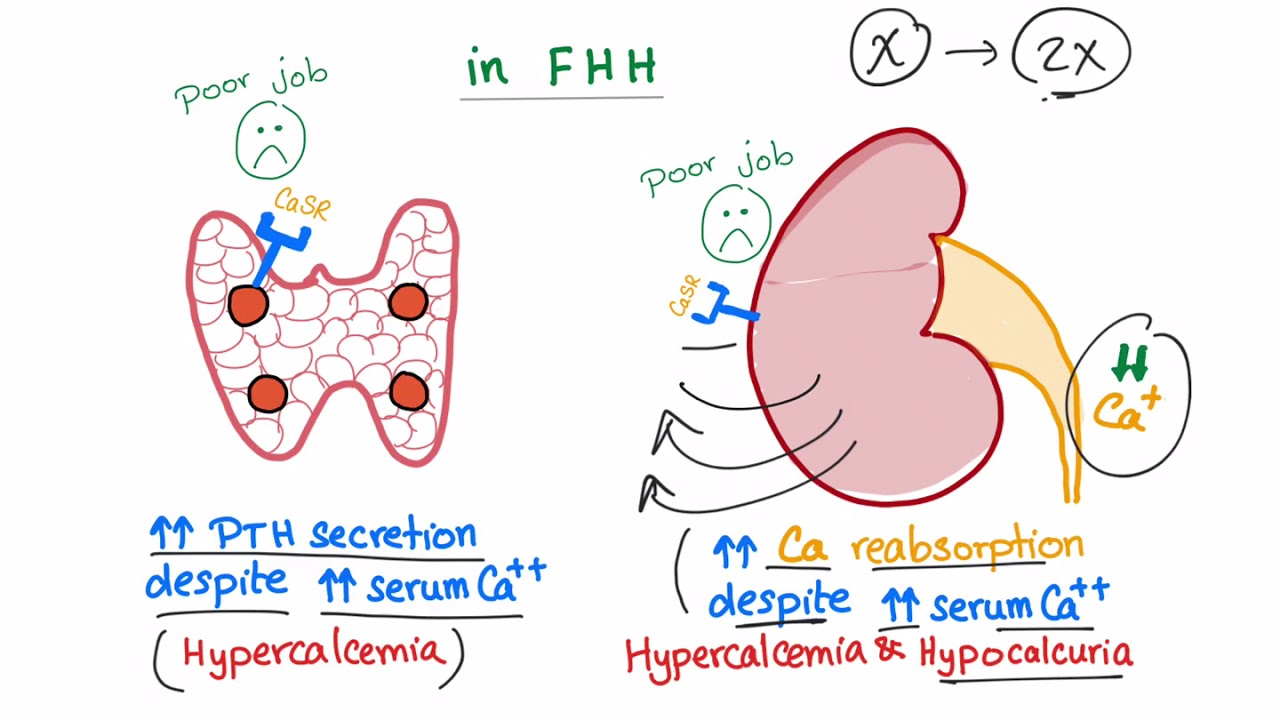
- Clinical features
- Usually asymptomatic
- Neonatal hypocalcemia in children of mothers with FHH (e.g., paresthesias, muscle spasms, seizures)
- Diagnosis
- Key Labs:
- Mildly elevated serum Ca (usually < 12 mg/dL).
- Normal to mildly elevated PTH (inappropriate in the setting of hypercalcemia).
- Low 24-hour urine Ca excretion (< 100 mg/24h).
- Confirmatory/Gold Standard:
- Urine Calcium-to-Creatinine Clearance Ratio (UCCR): < 0.01 (UCCR = [Urine Ca × Serum Cr] / [Serum Ca × Urine Cr]). c
- Genetic testing for CASR gene mutations (used if UCCR is borderline between 0.01 and 0.02).
- Key Labs:
- Differential diagnostics
- Primary Hyperparathyroidism (PHPT):
- Diff by: UCCR > 0.02, high 24-hour urine Ca (> 200 mg/24h), and complications like nephrolithiasis or osteoporosis. c
- Humoral Hypercalcemia of Malignancy:
- Diff by: High serum Ca, suppressed PTH, elevated PTHrP, and severe systemic symptoms.
- Lithium-induced Hypercalcemia:
- Diff by: History of lithium use; mimics FHH by raising the set-point of CaSR.
- Primary Hyperparathyroidism (PHPT):
- Therapy
- No treatment necessary