Mutations in genes like ENG or ACVRL1 disrupt the TGF-β signaling pathway, essential for vascular integrity.
Leads to thin-walled vessels and direct connections between arteries and veins (Arteriovenous Malformations - AVMs) without intervening capillaries.
Clinical Features
Also known as Osler-Weber-Rendu syndrome.
Spontaneous, recurrent epistaxis is the most common presenting symptom, often starting in childhood.
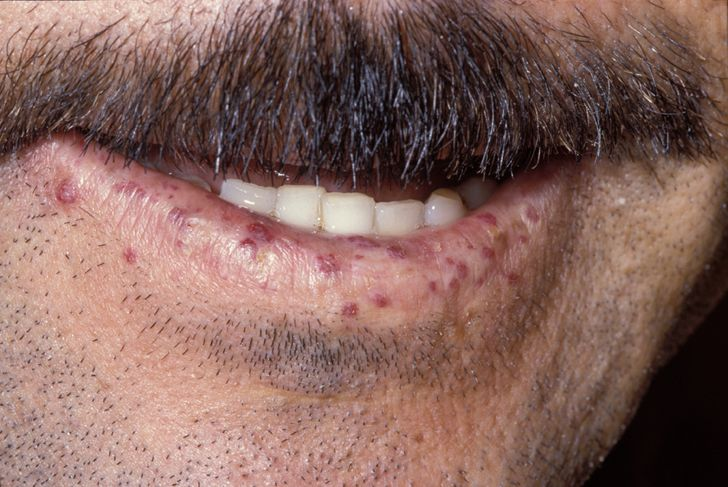
Mucocutaneous telangiectasias: small, red, blanchable lesions on lips, tongue, face, and fingers.
Visceral AVMs can affect lungs, brain, liver, and GI tract.
Symptoms of visceral involvement may include SOB, hemoptysis, headaches, seizures, or GI bleeding (often presenting as melena or iron deficiency anemia).
Dx
Based on the Curaçao criteria (definite diagnosis if ≥3 are present):
Spontaneous, recurrent epistaxis.
Multiple telangiectasias at characteristic sites (lips, oral cavity, fingers, nose).
Visceral AVMs (pulmonary, hepatic, cerebral, spinal, or GI).
First-degree relative with HHT.
Screening for visceral AVMs is crucial and may involve a bubble echo (for pulmonary AVMs), and CT/MRI of the abdomen and brain.
Genetic testing can confirm the diagnosis, especially in uncertain cases or for family screening.
Key Associations/Complications
Iron deficiency anemia from chronic blood loss is very common.
Pulmonary AVMs: Can lead to hypoxemia (due to right-to-left shunting) and are a major risk for paradoxical emboli, causing TIA/stroke or brain abscesses.
Cerebral AVMs: Risk of intracranial hemorrhage and seizures.
Hepatic AVMs: Can lead to high-output heart failure.
There is an increased risk of thrombosis, which can be exacerbated by iron deficiency.