- Dihydropyridine (DHPR) CCBs (nifedipine and amlodipine) primarily act on vascular smooth muscles.
- Dihydropyridines = Dilate vessels.
- Nodihydropyridine CCBs (verapamil > diltiazem) primarily act on the heart.
- Non-dihydropyridines = act on the Nodes and cardiac muscle
| Feature | Skeletal Muscle | Cardiac Muscle | Smooth Muscle |
|---|---|---|---|
| Coupling | Mechanical (Voltage-gated) | Ca2+-Induced Ca2+ Release (CICR) | Chem/Elec-mechanical |
| Ca2+ Source | Intracellular Only (SR) | Extracellular + Intracellular | Extracellular + Intracellular |
| Ca2+ Sensor | Troponin C | Troponin C | Calmodulin (No Troponin) |
| Key Channel | RyR1 (physically linked to DHPR) | RyR2 (activated 2+ Ca2+ influx) | IP3 Receptor / Ca2+ Channels |
| Contraction | Tropomyosin movement | Tropomyosin movement | Myosin Phosphorylation (MLCK) |
| Relaxation | SERCA (Constitutive) | SERCA (Phospholamban reg.) | Myosin Phosphatase (MLCP) |
| Affected by CCBs? | NO DHPR acts only as a voltage sensor, not a channel. | YES: Non-Dihydropyridines (Verapamil, Diltiazem) target cardiac L-type channels to ↓ contractility/HR. | YES: Dihydropyridines (Amlodipine, Nifedipine) target vascular smooth muscle L-type channels to cause vasodilation. |
Tip
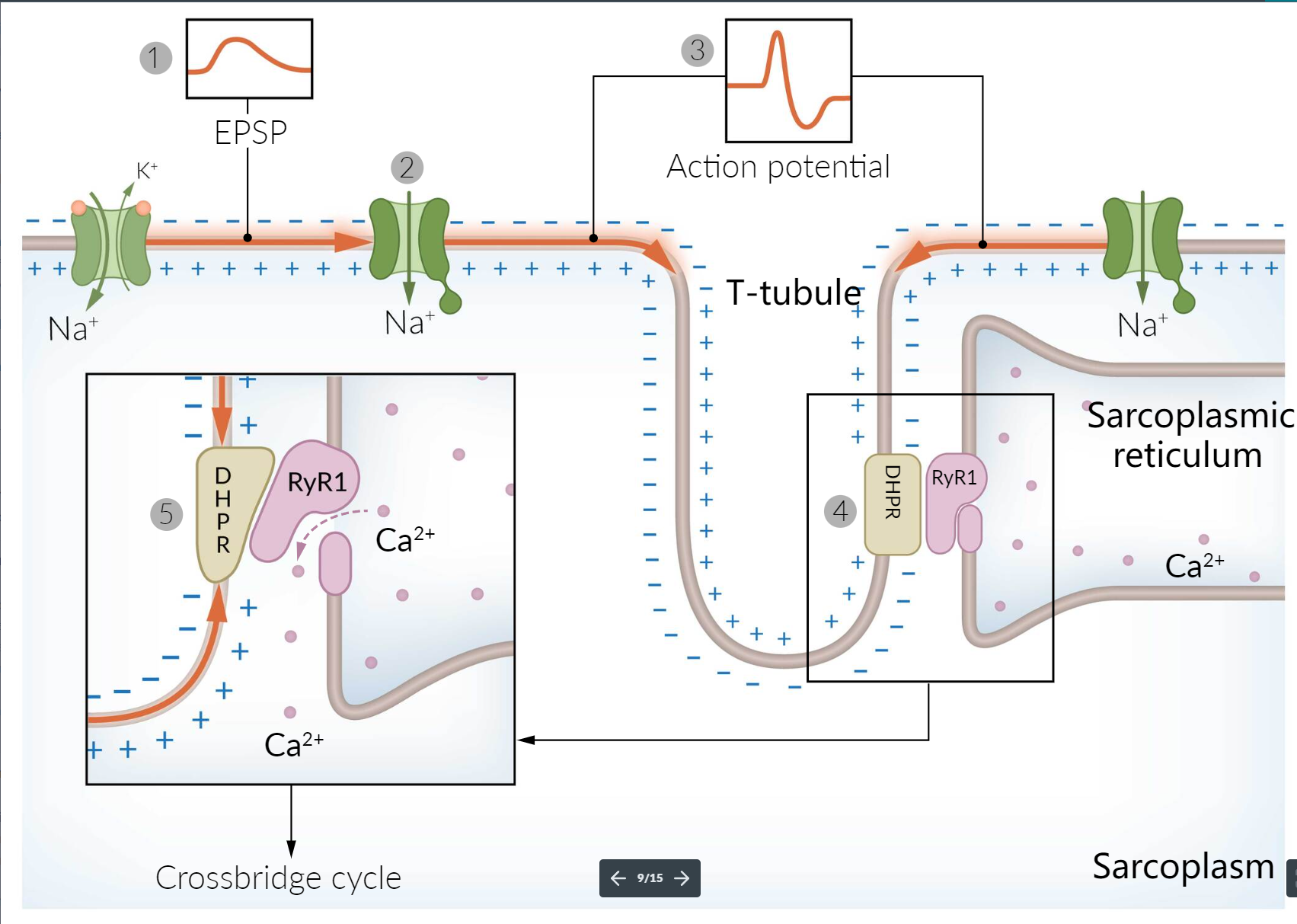
- Skeletal muscle: opening of voltage-sensitive dihydropyridine receptors (DHPR) in the T tubules and the mechanically coupled ryanodine receptors (RYR) in the SR → SR releases Ca2+ into the sarcoplasm (buffered by calsequestrin) → increased intracellular Ca2+
- CCBs can block an influx of extracellular calcium through DHPRs but cannot affect DHPR voltage-sensing capabilities or the resulting intracellular calcium release.
- Smooth muscle: stimulus opens L-type voltage-gated Ca2+ channels in the sarcolemma → influx of Ca2+ from the extracellular space into the smooth muscle cell (Ca2+ is also released from the SR, further increasing the intracellular concentration of Ca2+)
- Cardiac muscle: AP originating from the cardiac pacemaker cells → muscle cell depolarization that diffuses across the sarcolemma and into T-tubules → short, rapid influx of sodium; prolonged Ca2+ influx (via L-type Ca2+ channels) → Ca2+-induced Ca2+ release from the SR → increased intracellular Ca2+
- Therefore, both smooth muscle and cardiac muscle can be affected by CCBs because they rely on extracellular Ca2+ influx
Adverse effects
Dihydropyridines
- Effects due to vasodilation
- Peripheral edema (esp. amlodipine): can be reduced by adding a renin-angiotensin system antagonist (ACEI or ARB). c
- Development of peripheral edema is related to preferential dilation of precapillary vessels (arteriolar dilation), which leads to increased capillary hydrostatic pressure and fluid extravasation into the interstitium.
- ACEI/ARB can cause postcapillary venodilation and can normalize the increased capillary hydrostatic pressure, reducing the risk of peripheral edema in patients taking calcium channel blockers.
- Headaches, dizziness
- Facial flushing, feeling of warmth
- Reflex tachycardia
- Peripheral edema (esp. amlodipine): can be reduced by adding a renin-angiotensin system antagonist (ACEI or ARB). c
- Gingival hyperplasia
Nondihydropyridines
- Reduced contractility
- Verapamil decreases the amount of intracellular calcium available for excitation-contraction coupling within cardiac myocytes. This reduces myocardial contractility, which can be harmful in patients with impaired ventricular function.