- Definition & Associations
- Also known as Samter’s Triad (Classic USMLE triad):
- Asthma
- Chronic Rhinosinusitis with Nasal Polyps
- Hypersensitivity to Aspirin/NSAIDs
- Not an IgE-mediated reaction (Pseudoallergy).
- Pathophysiology
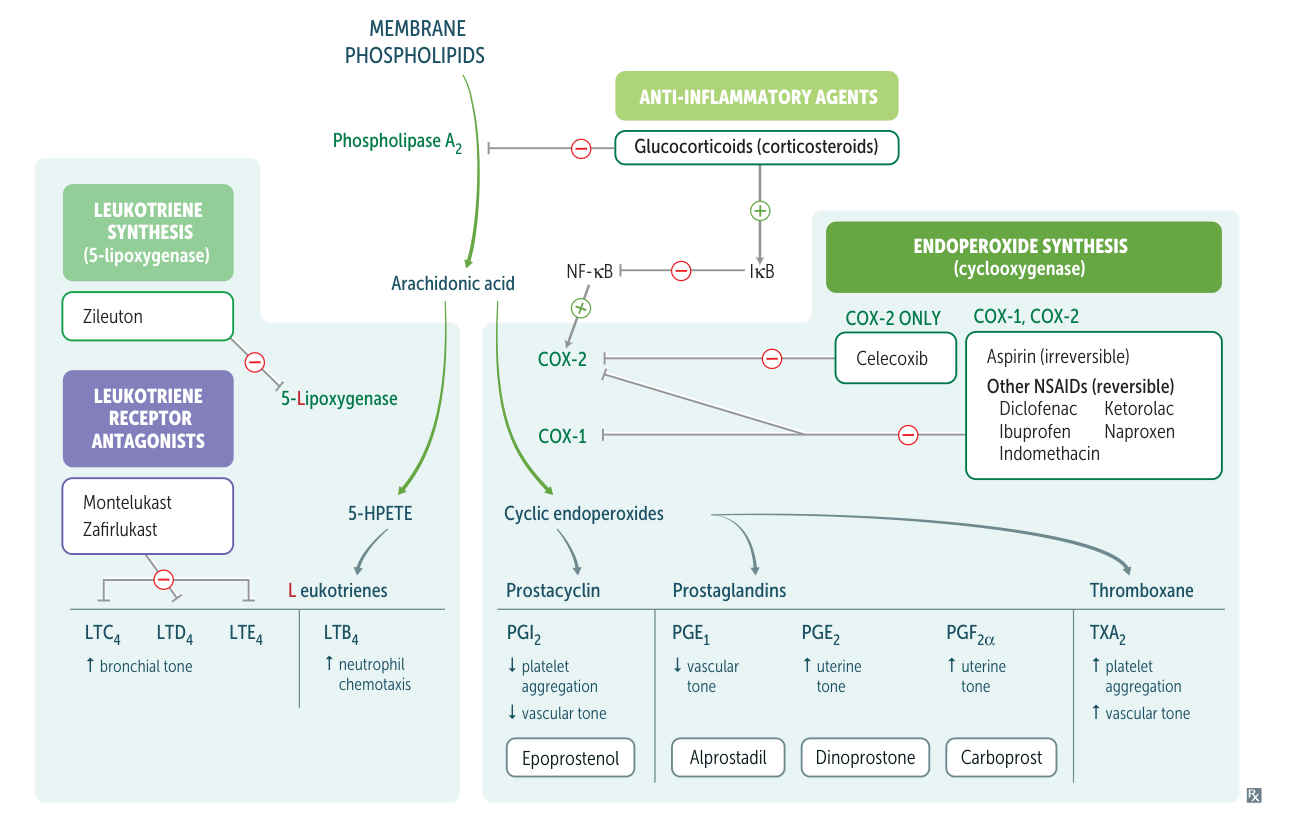
- Mechanism: Dysregulation of arachidonic acid metabolism.
- COX-1 inhibition by Aspirin/NSAIDs removes the “brake” on the 5-lipoxygenase (5-LOX) pathway.
- Result: Shunting of arachidonic acid towards leukotriene production.
- ↑ Cysteinyl Leukotrienes (LTC4, LTD4, LTE4): Potent bronchoconstrictors and promoters of vascular permeability/mucus production. t
- ↓ PGE2: Loss of anti-inflammatory prostaglandin that typically inhibits 5-LOX.
- Clinical Features
- Patient Profile: Adult-onset asthma, chronic congestion, anosmia (loss of smell).
- Reaction: Ingestion of Aspirin or COX-1 inhibiting NSAIDs triggers acute symptoms within 30 mins to 3 hours:
- Severe bronchospasm (wheezing, chest tightness)
- Rhinorrhea/congestion
- Facial flushing
- Nasal Polyps: Often visualized on physical exam (pale, gray, teardrop-shaped growths in nasal cavity).
- Diagnosis
- Primarily clinical based on history (The Triad).
- Aspirin Challenge: Gold standard (performed under medical supervision) but rarely required if history is classic.
- CT Sinuses: Shows pansinusitis and polyposis.
- Treatment & Management
- Avoidance: Strictly avoid Aspirin and all NSAIDs (use Acetaminophen or COX-2 inhibitors like Celecoxib cautiously).
- Pharmacotherapy:
- Leukotriene receptor antagonists (LTRAs): Montelukast, Zafirlukast (Target the pathway directly).
- 5-LOX Inhibitors: Zileuton (Blocks leukotriene synthesis).
- Biologics: Dupilumab (anti-IL-4/IL-13) or Omalizumab (anti-IgE) for severe refractory polyps/asthma.
- Aspirin Desensitization:
- Indicated if the patient requires aspirin for cardiovascular/cerebrovascular protection or if symptoms are refractory to medical management.
- Involves gradual administration of increasing aspirin doses to deplete leukotrienes.
- Surgery: Endoscopic sinus surgery (polypectomy) for symptomatic relief (recurrence is common).