Mechanism: Mucociliary clearance moves mucus toward the ostia.
Primary Ciliary Dyskinesia (Kartagener Syndrome): Defect in dynein arm → immotile cilia → chronic sinusitis, bronchiectasis, situs inversus, infertility.
Sinusitis
Definition & Etiology
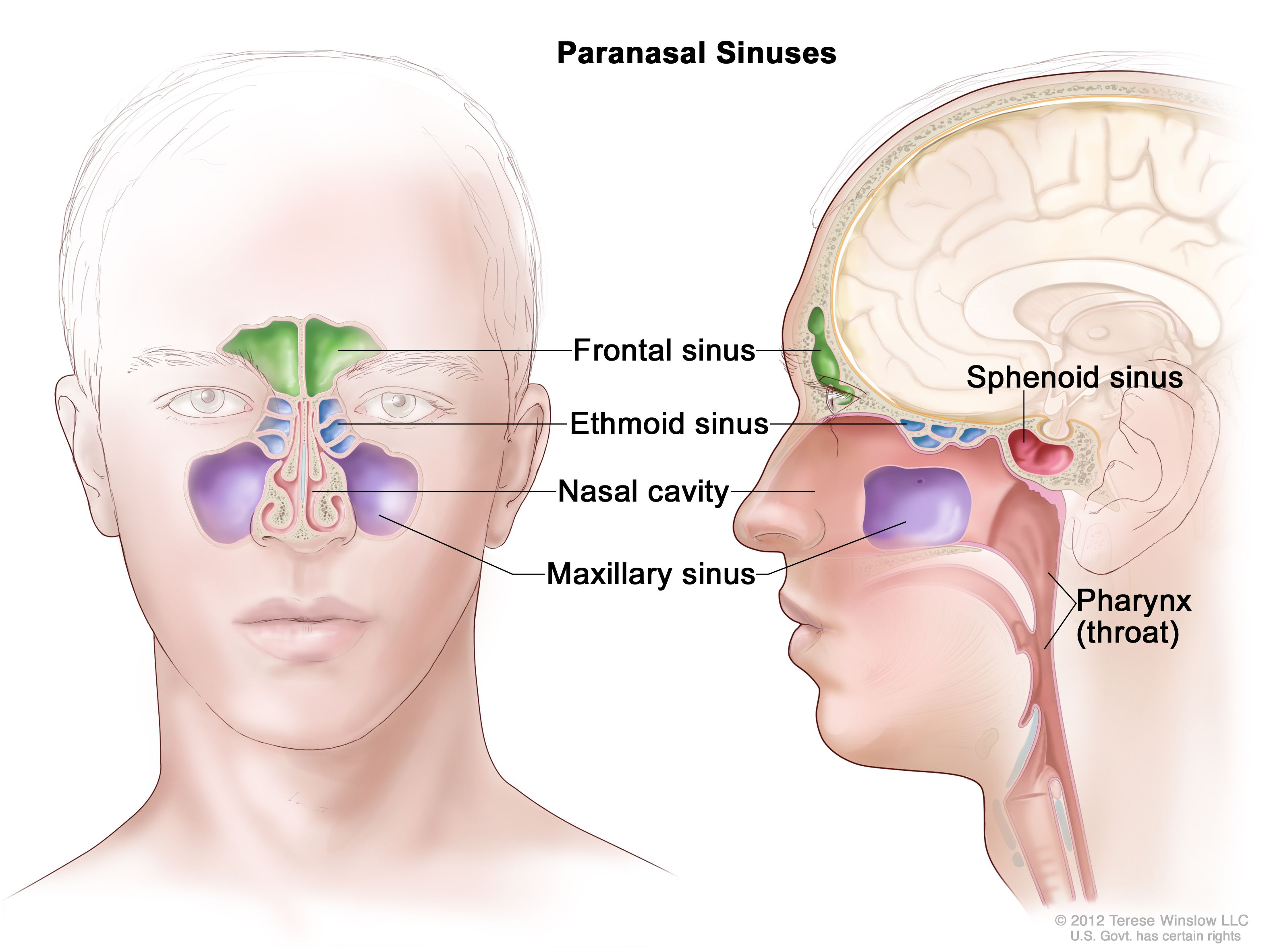
Inflammation of the paranasal sinuses, almost always involving the nasal mucosa (hence, “rhinosinusitis”).
Acute (<4 weeks):Most commonly viral (e.g., Rhinovirus, Influenza), often following a URI. A small percentage (0.5-2%) develop a secondary bacterial infection.
Acute Bacterial Pathogens: Most common are Streptococcus pneumoniae, Haemophilus influenzae (non-typeable), and Moraxella catarrhalis.
Chronic (>12 weeks): Often involves S. aureus, anaerobes, and gram-negative bacteria. Fungal causes (e.g., Aspergillus, Mucor) are significant in immunocompromised patients (e.g., diabetics, neutropenic).
Pathophysiology: The maxillary sinus is the largest of the paranasal sinuses. Its drainage ostium is located superiorly and medially, which leads to inefficient, gravity-dependent drainage. This predisposition to stasis makes it the most susceptible to infection.
Clinical Presentation
Symptoms: Nasal congestion, purulent (yellow-green) nasal discharge, facial pain/pressure (worse on bending forward), maxillary toothache, fever, and cough.
Differentiating Viral vs. Bacterial:
Viral: Symptoms typically last <10 days and are self-improving.
Bacterial: Suspect if symptoms persist >10 days without improvement, are severe from onset (fever ≥39°C/102.2°F + purulent discharge >3 days), or show a “double-sickening” course (worsening after initial improvement).
Viral turns to bacterial: Symptoms typically remain stable or improve for 5–6 days and then worsen (double worsening).
Diagnosis
Primarily clinical: Based on the duration and pattern of symptoms.
Physical Exam: Tenderness to palpation over sinuses, purulent drainage in the nasal cavity.
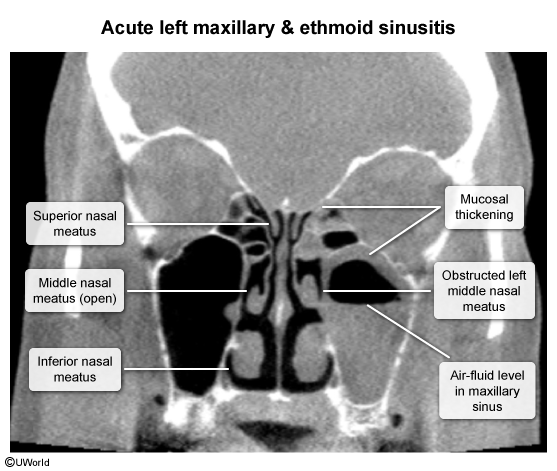
Imaging:Not recommended for uncomplicated acute sinusitis. A CT scan is the test of choice if complications (e.g., orbital, intracranial) are suspected or for chronic sinusitis evaluation.
Differential Diagnostics
Allergic Rhinitis: Associated with clear rhinorrhea, sneezing, itchy/watery eyes, and pale/boggy nasal mucosa.
Migraine/Tension Headache: Lacks purulent discharge and fever.
Dental Abscess: Can cause maxillary pain and focal swelling.
Management
Viral / Symptomatic Tx:
Analgesics (NSAIDs, acetaminophen).
Saline nasal irrigation and intranasal corticosteroids (e.g., fluticasone) can relieve congestion and facial pain.
Decongestants (oral or topical) for short-term use (<3-5 days) to avoid rebound congestion.
Bacterial Tx:
First-line antibiotic:Amoxicillin with or without clavulanate.
Indicated only if criteria for bacterial sinusitis are met (persistent, severe, or worsening course).
Macrolides and fluoroquinolones are generally discouraged due to resistance and adverse effects.
Key Associations & Complications
Complications are rare but serious and occur via direct extension of infection.
Orbital Cellulitis: Proptosis, pain with eye movements, vision changes. Most common complication, especially from ethmoid sinusitis.
Intracranial Extension: Can lead to meningitis, epidural abscess, or cavernous sinus thrombosis. Suspect with severe headache, fever, vision changes, or altered mental status.
Pott’s Puffy Tumor: Osteomyelitis of the frontal bone, presenting as a tender, doughy forehead swelling.
Invasive Fungal Sinusitis: A medical emergency in immunocompromised patients (especially DKA), often caused by Mucor or Aspergillus. Look for necrotic eschars in the nasal cavity.