Epidemiology
Etiology
- Microvascular damage (diabetes, hypertension, arteriosclerosis)
- Cavernous sinus thrombosis
Pathophysiology
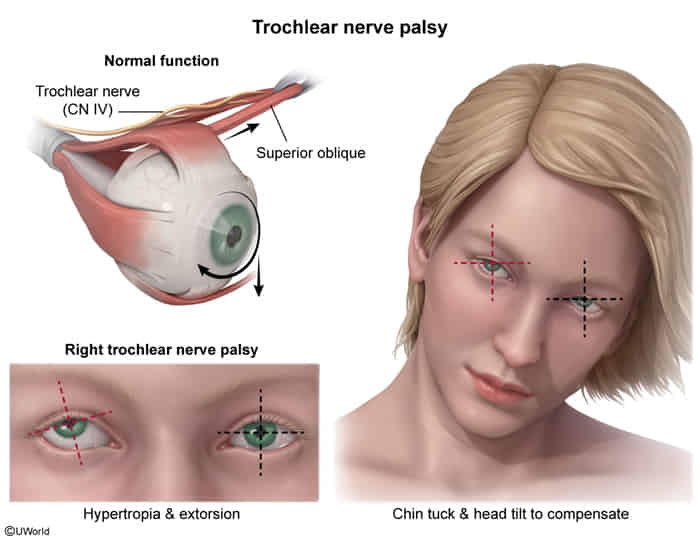
The direct antagonist of the Superior Oblique is the Inferior Oblique. When the SO is paralyzed (CN IV Palsy), the Inferior Oblique is left unopposed and pulls the eye into its own field of action.
- Superior Oblique (SO) Normal Action: Depression, Intorsion, Abduction.
- “S.O. Sinks Out”: The Superior Oblique makes the eye go Down (Sinks) and Out (Abduction).
- Inferior Oblique (IO) Normal Action: Elevation, Extorsion, Abduction.
The inferior oblique becomes unopposed, making the eye deviates upward and outward (extorted).
Clinical features
- Vertical or oblique diplopia
- Exacerbated on downgaze (e.g., reading, walking downstairs) away from side of affected muscle
- Worsens when patient turns the head towards the paralyzed muscle → compensatory head tilt to the opposite side of the lesion
Mnemonic
With damage to the CN IV, you cannot look at the floor.