Cranial nerve pathways
| 1 | Come | Cribiform plate |
|---|---|---|
| 2 | On | Optic Canal |
| 3 | Sofia | Superior Orbital Fissure |
| 4 | Sofia | Superior Orbital Fissure |
| 5.1 | Sofia | Superior Orbital Fissure |
| 5.2 | Right | Foramen Rotundum → Infraorbital foramen |
| 5.3 | On | Foramen Ovale → Mental foramen |
| 6 | Sofia | Superior Orbital Fissure |
| 7 | I’m | Internal Acoustic Meatus |
| 8 | Into | Internal Acoustic Meatus |
| 9 | Just | Jugular Foramen |
| 10 | Jiggly | Jugular Foramen |
| 11 | Juggs | Jugular Foramen |
| 12 | Honey | Hypoglossal Canal |
**All cranial nerves are PNS, EXCEPT for CN I and CN II, ** which are not true peripheral nerves but are considered tracts, or extensions, of the brain itself.
Course of cranial nerves
- Cortical Input (UMN): Most cranial nerve nuclei receive bilateral corticobulbar input. (Exception: CN VII low, CN XII)
- Significance: Unilateral cortical lesions (e.g., MCA stroke) usually do not cause significant deficits for these nerves (e.g., CN V, IX, X) because the healthy hemisphere compensates.
- Nuclear Output (LMN): Most cranial nerve nuclei innervate ipsilateral muscles. (Exception: CN IV)
- The Major Exception (CN IV):
- Trochlear Nerve (CN IV) is the only CN to decussate inside the brainstem before exiting.
- It is also the only CN to exit dorsally.
- The Sensory Exception (CN II):
- Optic Nerve (CN II) has partial decussation at the Optic Chiasm (nasal fibers cross).
- Cortical Control (UMN) Exceptions:
- Most CN nuclei receive bilateral input from the cortex.
- Exceptions (Contralateral input only):
- CN VII (Lower Face): UMN lesion Contralateral lower facial droop (forehead spared).
- CN XII (Geniohyoid): UMN lesion Tongue deviates to contralateral side.
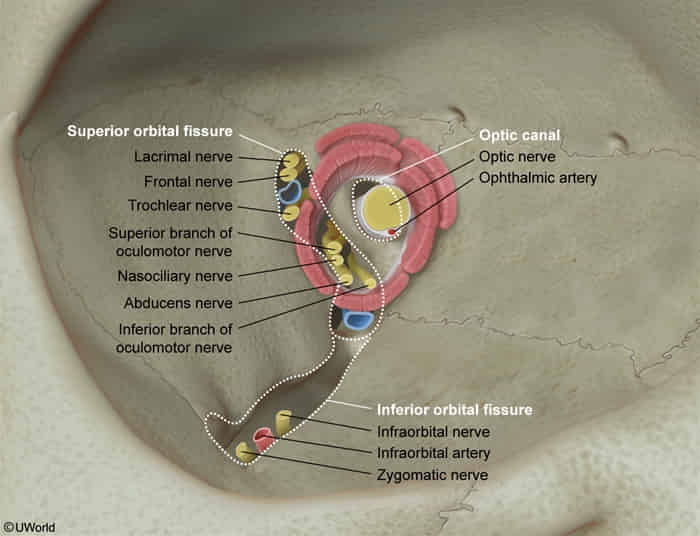
Around eyes
Tongue nerve intervention
- Motor innervation of the tongue is provided by the hypoglossal nerve (cranial nerve CN XII) with the exception of the palatoglossus muscle, which is innervated by the vagus nerve (CN X).
- General sensory innervation of the tongue (including touch, pain, pressure, and temperature sensation) is provided by:
- Anterior 2/3 of the tongue: mandibular branch of trigeminal nerve (CN V3) t
- Posterior 1/3 of the tongue: glossopharyngeal nerve (CN IX)
- Posterior area of the tongue root: vagus nerve (CN X)
- Gustatory innervation (taste buds) is as follows:
- Anterior 2/3 of the tongue: chorda tympani branch of facial nerve (CN VII)
- Posterior 1/3 of the tongue: glossopharyngeal nerve (CN IX)
- Posterior area of the tongue root and taste buds of the larynx and upper esophagus: vagus nerve (CN X)
Lesion localization
| Function | Brainstem Nucleus Innervation | Pathway Example |
|---|---|---|
| Most Cranial Nerves | Bilateral | Left Hemisphere → Right & Left Nuclei |
| Lower Face (CN VII) | Contralateral | Left Hemisphere → Right Lower Face Nucleus → Right Lower Face Muscles |
| Tongue (CN XII) | Contralateral | Left Hemisphere → Right Hypoglossal Nucleus → Right Tongue Muscles |
- Most cranial nerve nucleus receive bilateral upper motor neuron (supranuclear) innervation, except for:
- CN VII (lower face): The motor nucleus for the lower face receives only contralateral cortical input. This is why a UMN lesion (e.g., stroke) causes contralateral paralysis of the lower face only, with sparing of the forehead (which is bilaterally innervated).
- CN XI (partially): The spinal accessory nerve’s innervation of the trapezius muscle is predominantly contralateral. A UMN lesion can lead to contralateral trapezius weakness. Innervation to the sternocleidomastoid muscle is primarily ipsilateral.
- CN XII (partially): The hypoglossal nerve’s innervation to the genioglossus muscle (responsible for tongue protrusion) is predominantly contralateral. A UMN lesion causes the tongue to deviate away from the side of the lesion upon protrusion.
- Most cranial nerves do not decussate after their nucleus, except for:
- CN IV (Trochlear Nerve): This is the major exception. The nerve fibers of CN IV decussate (cross) within the midbrain at the superior medullary velum before exiting the brainstem dorsally. This means the right trochlear nucleus controls the left superior oblique muscle, and vice versa.
Cranial nerve reflexes
| Reflex | Afferent (Sensory) Limb | Efferent (Motor) Limb |
|---|---|---|
| Pupillary Light | CN II (Optic) | CN III (Oculomotor) (Parasympathetics via Edinger-Westphal) |
| Corneal (Blink) | CN V1 (Ophthalmic) | CN VII (Facial) (Temporal branch) |
| Jaw Jerk | CN V3 (Mandibular) (Muscle spindle sensory) | CN V3 (Mandibular) (Motor) |
| Vestibulo-ocular | CN VIII (Vestibular) | CN III, IV, VI |
| Carotid Sinus | CN IX (Glossopharyngeal) | CN X (Vagus) |
| Gag (Pharyngeal) | CN IX (Glossopharyngeal) | CN X (Vagus) |
| Cough | CN X (Vagus) (Internal laryngeal n.) | CN X (Vagus) (Recurrent laryngeal n.) + Phrenic/Spinal |
| Lacrimation | CN V1 (Ophthalmic) | CN VII (Facial) |