Epidemiology
Etiology
Pathophysiology
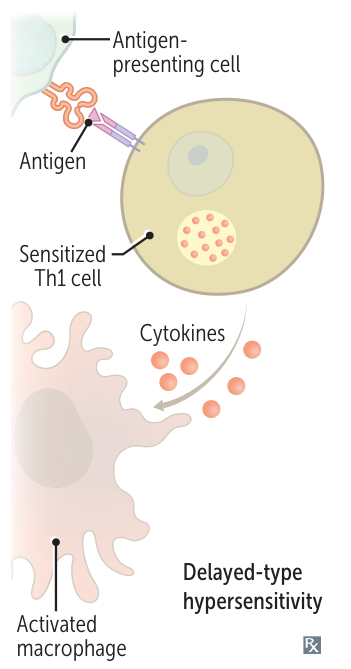
Compared to type I-III hypersensitivity reactions, which are antibody-mediated, type IV reactions are mediated by T cells. Type IV hypersensitivity reactions involve two major steps:
- Sensitization Phase: Initial exposure to antigen antigen processed by Langerhans cells/APCs presented to CD4+ T cells in lymph nodes clonal expansion of T cells.
- Effector Phase (Re-exposure):
- CD4+ Th1 response: Release cytokines (IFN-γ, IL-2).
- CD8+ T cell response: Direct cytotoxicity (perforin/granzyme) against target cells (e.g., viral-infected cells, contact dermatitis).
Examples
- Skin tests
- Candida skin test (to test the immune function of T cells)
- A diagnostic test in which Candida albicans antigen is injected intradermally to the arm. The injection site is examined 48 hours later. Induration ≥5 mm in diameter is considered a positive reaction and indicates prior exposure to antigen and an intact immune response mediated by T cells.
- This test requires patients to have encountered Candida before. Luckily, nearly everyone encounters Candida at some point in their lives.
- Mantoux tuberculin skin test for latent tuberculosis
- Candida skin test (to test the immune function of T cells)
- Exanthematous drug eruption: morbilliform rash on the trunk and proximal extremities
- Associated symptoms include pruritus and low-grade fever

- Typical onset 5-14 days after drug exposure
- Caused by anticonvulsants, antibiotics, antiretroviral therapy
- Most commonly caused by antibiotics, e.g., “ampicillin rash” following ampicillin administration for infectious mononucleosis
- Resolves after discontinuation of the offending drug
- Associated symptoms include pruritus and low-grade fever