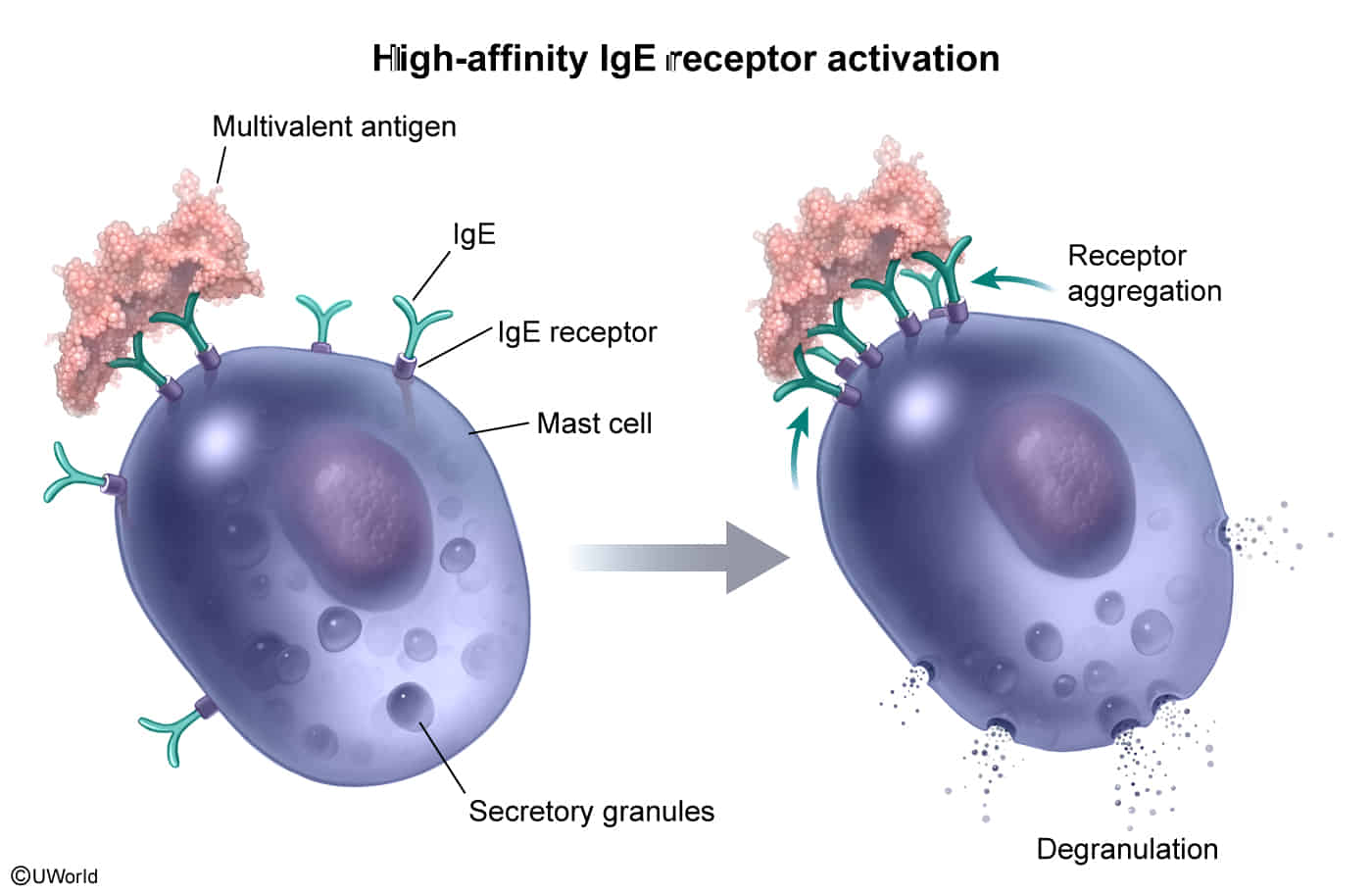
When a multivalent antigen comes in contact with the cell, multiple IgE antibodies become cross-linked, resulting in aggregation of the FcεRI receptors on the mast cell surface.
This clumping of receptors leads to the activation of non-receptor tyrosine kinases, triggering an intracellular cascade that ultimately results in mast cell and basophil degranulation.
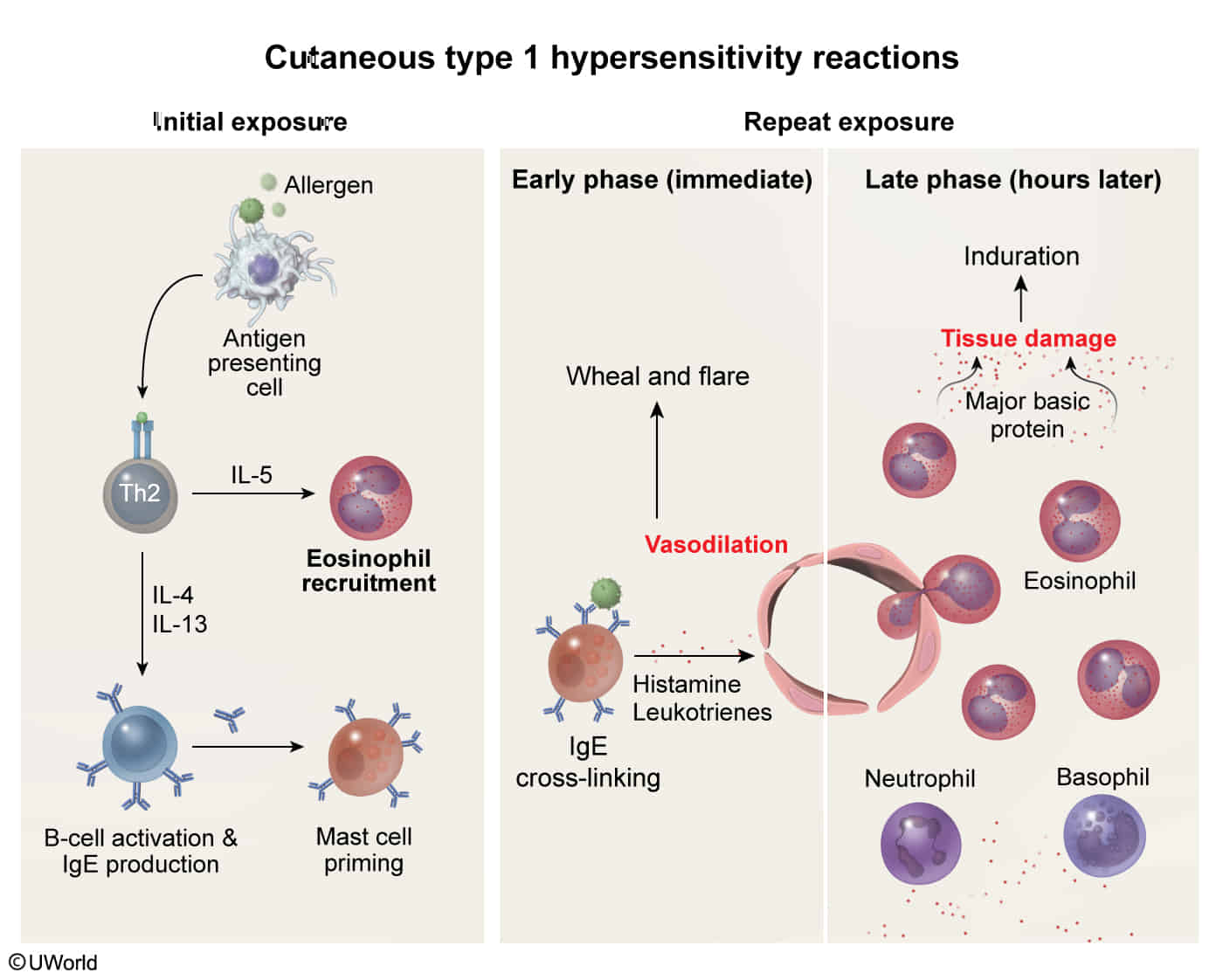
Cytokines (e.g., TNF-α, IL-5): Recruit and activate other inflammatory cells.
IL-5 is the key chemotactic factor for eosinophils.
Eosinophils are recruited and release their granule contents, including Major Basic Protein (MBP), which is cytotoxic to epithelial cells and contributes to the chronic tissue damage seen in conditions like asthma.
Clinical features
Diagnostics
Hypersensitivity blood tests (in vitro)
Tryptase
A relatively specific marker of mast cell activation
Elevated levels indicate an increased risk of severe reactions.
Treatment
Long-term Management & Prophylaxis
Avoidance: Identification and removal of triggers (food, dander, pollen).
Immunotherapy (Desensitization):
Repeated low-dose exposure to antigen.
Induces production of IgG4 (“blocking antibody”) which intercepts antigen before it binds IgE on mast cells.
Mast Cell Stabilizers: Cromolyn sodium (prevents mast cell degranulation; used for prophylaxis only, not acute Sx).
Leukotriene Receptor Antagonists: Montelukast, Zafirlukast (good for aspirin-induced asthma).
Monoclonal Antibodies:
Omalizumab: Anti-IgE antibody. Binds free serum IgE, preventing attachment to Fcϵ\epsilonϵRI on mast cells/basophils. Indicated for severe, persistent allergic asthma.