Rapid-onset, non-pitting, asymmetric edema of subQ and submucosal tissues.
Common sites: Face, lips, tongue, larynx, extremities, genitals.
GI Tract: Intestinal wall edema causes severe, colicky abdominal pain, N/V, and watery diarrhea (often mimics acute abdomen).
Key Distinction:
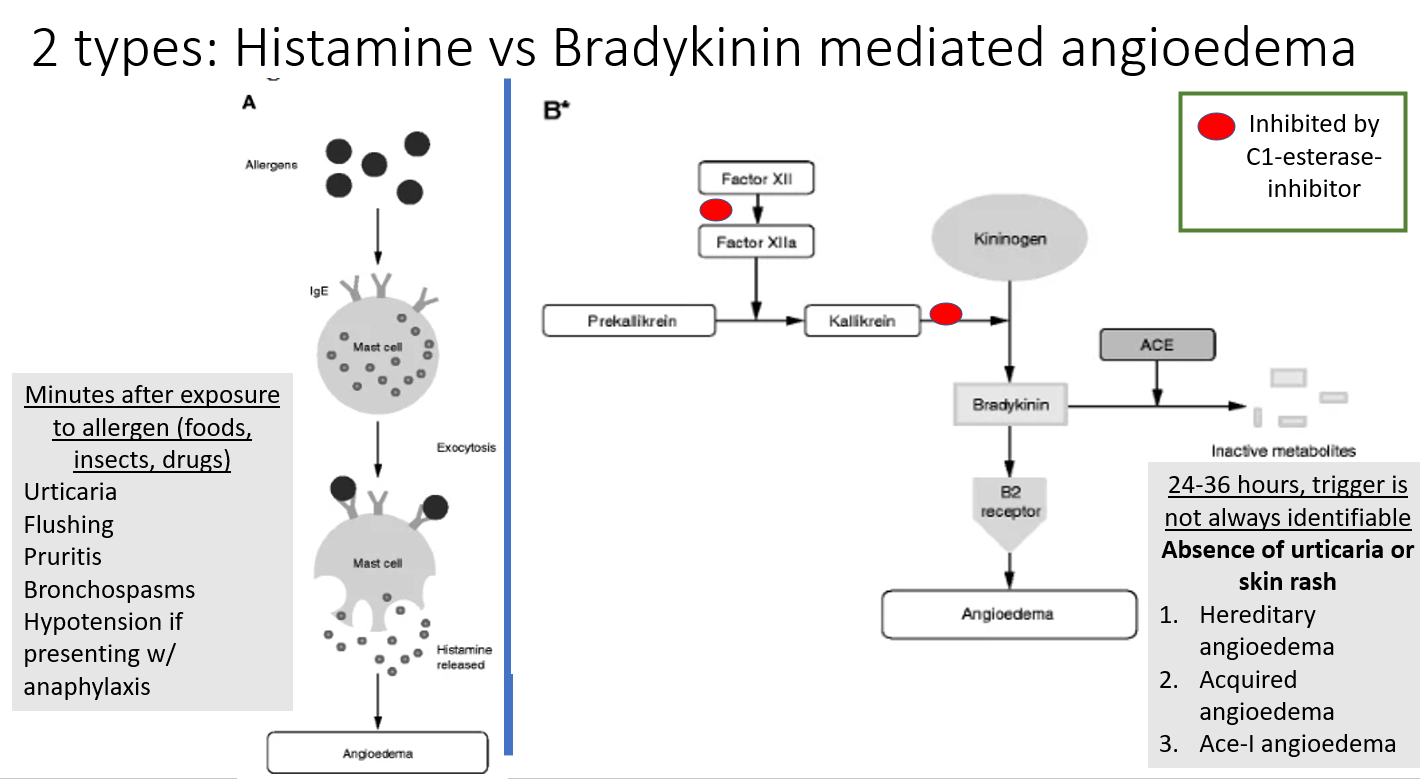
Mast cell-mediated: Accompanied by urticaria (hives), pruritus, flushing, bronchospasm, or hypotension.
Bradykinin-mediated: NO urticaria, NO pruritus.
Management
Emergency Stabilization (Airway): Monitor strictly. Early intubation if stridor, voice changes, or significant laryngeal/tongue edema. (Surgical airway/cricothyrotomy if intubation fails). c
Discontinue offending agent: Stop ACEi immediately (and avoid ARBs, though risk is lower).
Targeted Pharmacotherapy:
Mast cell-mediated: IM Epinephrine (first-line for anaphylaxis), H1/H2 blockers, systemic glucocorticoids.
Bradykinin-mediated (HAE/ACEi):
First-line: Icatibant (Bradykinin B2 receptor antagonist) or Ecallantide (Kallikrein inhibitor) or Purified C1 INH concentrate.
Second-line: Fresh Frozen Plasma (FFP) if specific agents are unavailable (contains kininase II which breaks down bradykinin).
Note: Epi, antihistamines, and steroids are INEFFECTIVE for bradykinin-mediated angioedema.
Prophylaxis (for HAE): Danazol (synthetic androgen) or C1 INH concentrate prior to dental work/surgery.