Caused by anterosuperior displacement of the infundibular septum.
Associated with 22q11 deletion syndromes (DiGeorge) and Down syndrome.
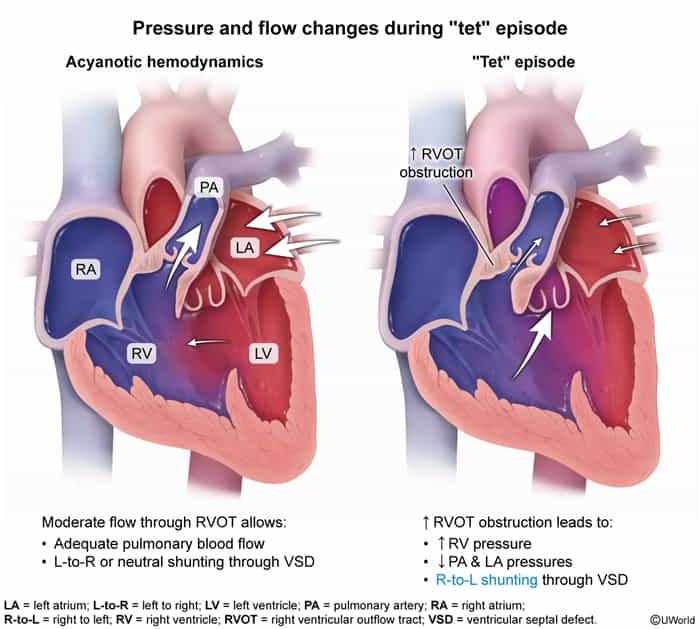
Pathophysiology
Pulmonary infundibular stenosis (Determine severity of cyanosis).
Right ventricular hypertrophy (RVH) – concentric, due to pressure overload.
Overriding aorta (sits over the VSD).
VSD (Ventricular Septal Defect) – usually large and non-restrictive.
Clinical features
Tet spells: intermittent hypercyanotic, hypoxic episodes with a peak incidence at 2–4 months after birth
Associated with psychological and physical stress (e.g., crying, feeding, defecation)
Caused by either an increase in pulmonary vascular resistance (PVR) or a decrease in systemic vascular resistance (SVR) → low SVR:PVR ratio allows the deoxygenated right ventricular output to take the low-resistance route to the systemic circulation, leading to acute hypoxemia (“Tet spell”).
Harsh crescendo-decrescendo systolic ejection murmur at the left upper sternal border
Caused by pulmonary stenosis, not the associated VSD
VSD is so large that no sound
Single S2
Possible RV heave and systolic thrill
Diagnostics
Increased hematocrit: secondary polycythemia
Treatment
Ductal-dependent CHDs: a group of CHDs that require the patent ductus arteriosus (PDA), which supplies either pulmonary or systemic circulation, to sustain life until surgery can be performed
PDA supplies systemic circulation in the following: