Turner Syndrome (45,XO): High association (up to 15% of cases).
Bicuspid Aortic Valve: Present in >50% of patients.
Intracranial Berry Aneurysms (risk of subarachnoid hemorrhage).
Pathophysiology
Narrowing (stenosis) of the aortic lumen.
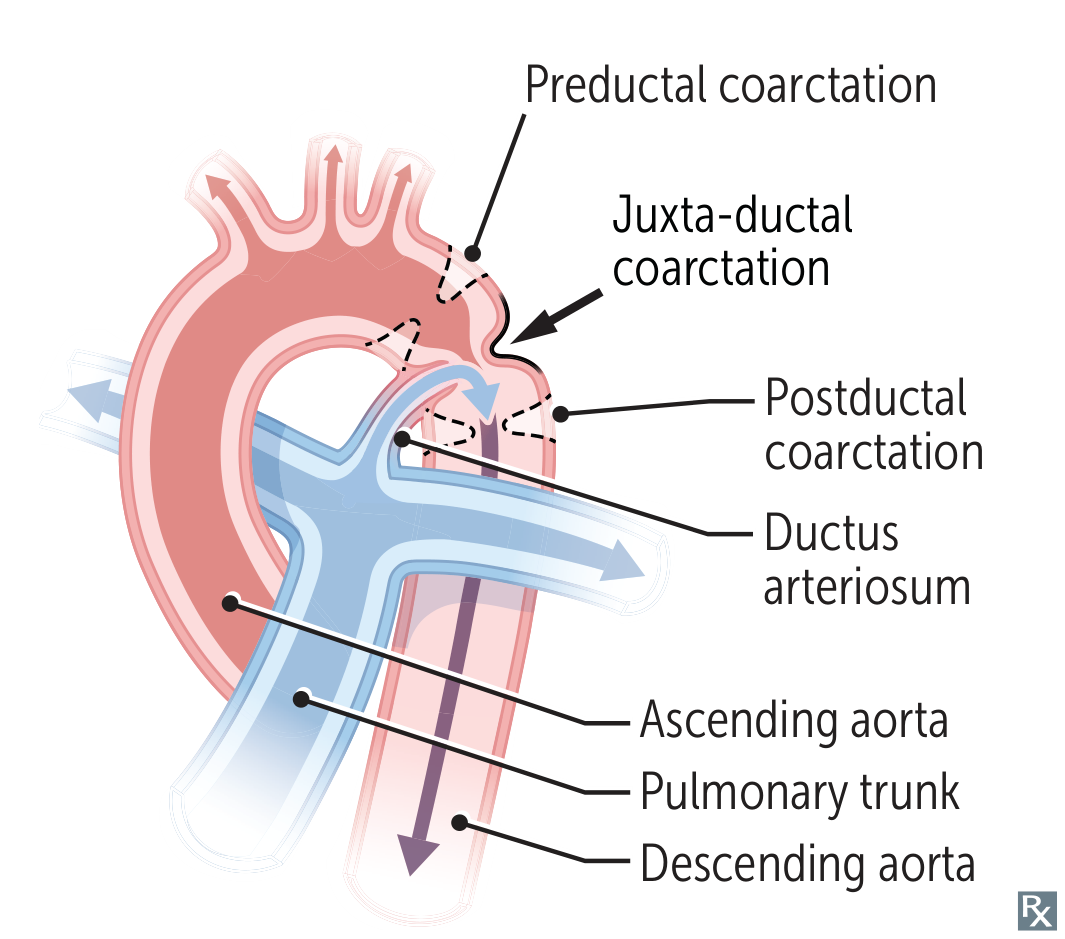
Infantile Type (Preductal): Stenosis proximal to the ductus arteriosus. Dependent on patent ductus arteriosus (PDA) for systemic perfusion.
Adult Type (Postductal): Stenosis distal to the ductus arteriosus (distal to left subclavian).
Clinical features
Neonatal (Pre-ductal):
Heart failure, poor feeding, and shock as the PDA closes (typically day 3-10 of life).
Differential cyanosis (cyanosis of the lower body, normal upper body).
Adult/Post-pediatric (Post-ductal):
Asymptomatic HTN: Often incidental finding.
Widened pulse pressure: The SBP shoots up heavily due to the physical narrowing and stiffening of the proximal aorta (mechanical), while the DBP is elevated due to the kidneys chronically pumping out renin in response to distal hypoperfusion (hormonal). c
UE vs. LE BP Differential: Systolic BP higher in arms than legs.
Brachial-femoral pulse delay.
Symptoms: Epistaxisc , headaches (due to UE HTN), or LE claudication (due to LE ischemia).
Auscultation
Midsystolic murmur heard best over the left interscapular area.
Continuous murmur in the left infraclavicular region and interscapular region c
Collateral Circulation: To bypass the obstruction, blood flows through enlarged collateral vessels, specifically the intercostal arteries.
Diagnostics
Initial Clinical Step: BP measurement in all four extremities.
Best Initial Imaging: Echocardiogram (TTE); visualizes the shelf-like narrowing and confirms pressure gradient.
Confirmatory/Gold Standard: Cardiac Catheterization (used if TTE is non-diagnostic or for pre-intervention planning).
CXR findings:
“3” Sign: Pre- and post-stenotic dilation of the aorta.
Rib Notching: Erosion of the inferior surface of the 3rd–8th ribs by dilated intercostal collateral arteries. c