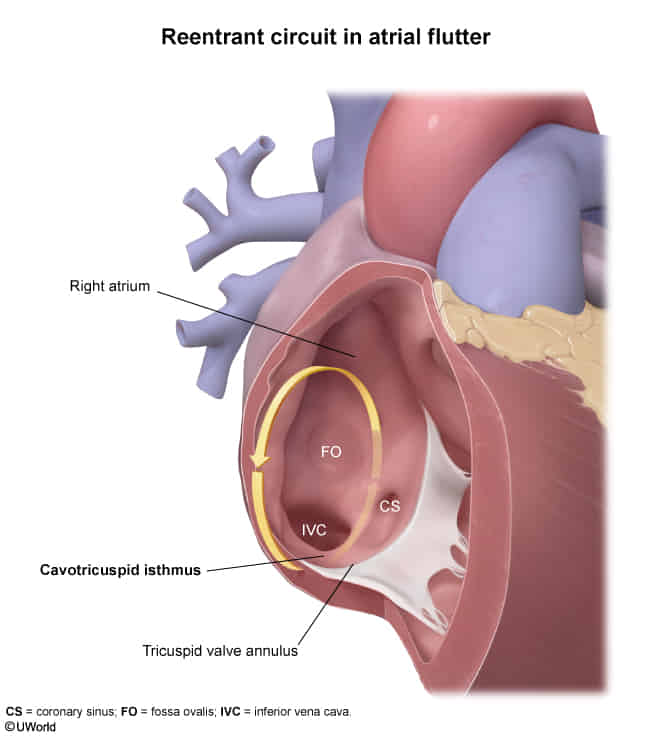
Type I (common; typical or isthmus-dependent flutter): caused by a counterclockwise (more common) or clockwise (less common) macroreentrant activation of cardiac muscle fibers in the right atrium that travels along the tricuspid annulus and passes through the cavotricuspid isthmus
Different from AFib, which originates from pulmonary vein ostia
Clinical features
Diagnostics
Atrial flutter vs atrial fibrillation
Feature
Atrial Flutter
Atrial Fibrillation
Site of Origin
Right Atrium (re-entrant circuit involving the cavotricuspid isthmus).
Left Atrium (ectopic foci, most commonly near the pulmonary vein ostia).
Pathophysiology
Organized macro-reentrant circuit.
Chaotic multiple atrial foci.
ECG Rhythm
Regular or regularly irregular.
Irregularly irregular.
Atrial Waves (ECG)
“Sawtooth” flutter waves (~300 bpm).
Fibrillatory waves (no P waves).
Management Pearl
Catheter ablation is highly curative.
Lifelong anticoagulation (CHA₂DS₂-VASc score) is key to prevent stroke.
ECG
Narrow complex tachycardia
Regular atrial activity at ~300 bpm
Loss of the isoelectric baseline
“Saw-tooth” pattern of inverted flutter waves in leads II, III, aVF
Anticlockwise Reentry: Commonest form of atrial flutter (90% of cases). Retrograde atrial conduction produces
Inverted flutter waves in leads II,III, aVF
Positive flutter waves in V1 — may resemble upright P waves
Upright flutter waves in V1 that may resemble P waves
Ventricular rate depends on AV conduction ratio (see below)
Atrial flutter will not usually cardiovert with these techniques (unlike AVNRT), although typically there will be a transient period of increased AV block during which flutter waves may be unmasked
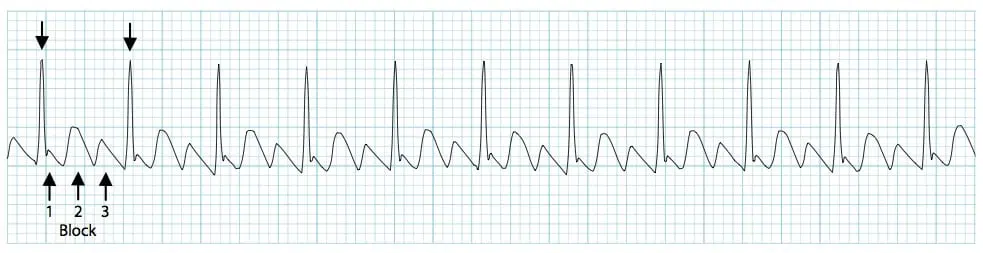
RR intervals
In atrial flutter with variable block the R-R intervals will be multiples of the P-P interval — e.g. assuming an atrial rate of 300bpm (P-P interval of 200 ms), the R-R interval would be 400 ms with 2:1 block, 600 ms with 3:1 block, and 800 ms with 4:1 block
Look for identical R-R intervals occurring sporadically along the rhythm strip; then look to see whether there is a mathematical relationship between the various R-R intervals on the ECG
In contrast, atrial fibrillation will be completely irregular, with no patterns to be discerned within the R-R intervals