- Epidemiology & Risk Factors
- Age: Toddlers (1–3 yrs) most common (incomplete dentition, immature swallowing).
- Anatomy: R main bronchus > L main bronchus (R is wider, shorter, and has a more vertical angle).
- RFs: Poor supervision, eating while playing, neurological impairment, dental procedures, small toys/nuts/seeds (organic FBs cause severe local chemical bronchitis).
- Clinical Features
- Acute presentation: Sudden-onset choking, coughing, gagging, cyanosis, or dyspnea.
- Subacute/Chronic presentation: Recurrent pneumonia, persistent croupy cough, localized wheezing unresponsive to bronchodilators.
- PE: Unilateral decreased breath sounds, localized wheezing, stridor (if laryngotracheal FB), inspiratory monophonic wheeze, hyperresonance to percussion on affected side.
- Diagnosis
- Initial: CXR (obtain inspiratory and expiratory films, or bilateral decubitus films in uncooperative peds).
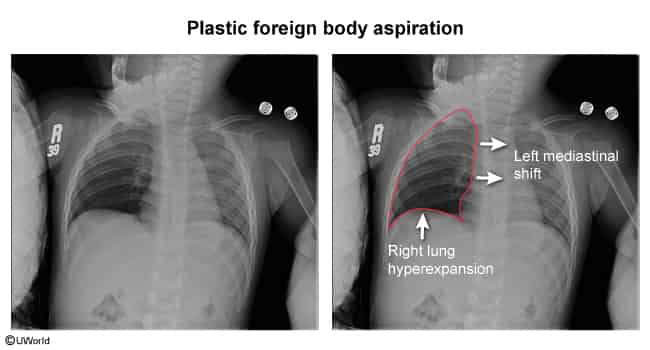
- Findings: Air trapping (hyperlucency/hyperinflation of affected lung on expiration due to ball-valve effect), atelectasis (if complete obstruction), mediastinal shift away from the affected side on expiration, radiopaque object (seen in <20% of cases, e.g., coins, batteries).
- Note: A normal CXR does not rule out FBA if clinical suspicion is high, because at least 30% of radiographs are normal, particularly if a radiolucent FB (eg, food) is lodged in a small airway.
- Confirmatory & Gold Standard: Rigid bronchoscopy (allows direct visualization, airway protection, and therapeutic intervention).
- Differential Diagnostics
- Asthma: Diff by recurrent episodes, bilateral wheezing, responsive to bronchodilators, history of atopy.
- Croup (Laryngotracheobronchitis): Diff by viral prodrome, barking cough, inspiratory stridor, “steeple sign” on AP neck X-ray.
- Epiglottitis: Diff by high fever, toxic appearance, drooling, dysphagia, distress, “thumbprint sign” on lateral neck X-ray.
- Bronchiolitis: Diff by age <2 yrs, RSV prodrome (runny nose, congestion), bilateral wheezing, diffuse CXR findings.
- Management
- 1. Acute Airway Obstruction (Emergency/Choking):
- Infants (<1 yr): 5 back blows followed by 5 chest thrusts. Repeat.
- Children (>1 yr) & Adults: Abdominal thrusts (Heimlich maneuver).
- Unresponsive/Unconscious: Start CPR. Inspect airway for visible FB before rescue breaths (no blind finger sweeps).
- 2. Stable Patient (Partial/Suspected Obstruction):
- First-line: Rigid bronchoscopy under general anesthesia (preferred in peds for airway control and extraction).
- Alternative/Adults: Flexible bronchoscopy (used if FB is distal, or for initial diagnosis in adults prior to rigid extraction).
- Special Case: Esophageal button battery requires immediate endoscopic removal to prevent liquefactive necrosis and tracheoesophageal fistula (TEF) formation.
- Complications
- Post-obstructive/recurrent pneumonia or lung abscess.
- Atelectasis.
- Bronchiectasis (if FB is retained chronically).
- Pneumothorax or pneumomediastinum.
- Bronchial stenosis or granulation tissue formation.