- Epidemiology & Risk Factors
- Source: Most commonly odontogenic infection (infection of 2nd/3rd lower molars; ~90% of cases).
- Risk Factors: Poor dental hygiene, recent dental extraction, DM, immunosuppression.
- Microbiology: Polymicrobial (viridans streptococci, oral anaerobes like Peptostreptococcus, Bacteroides).
- Clinical Features
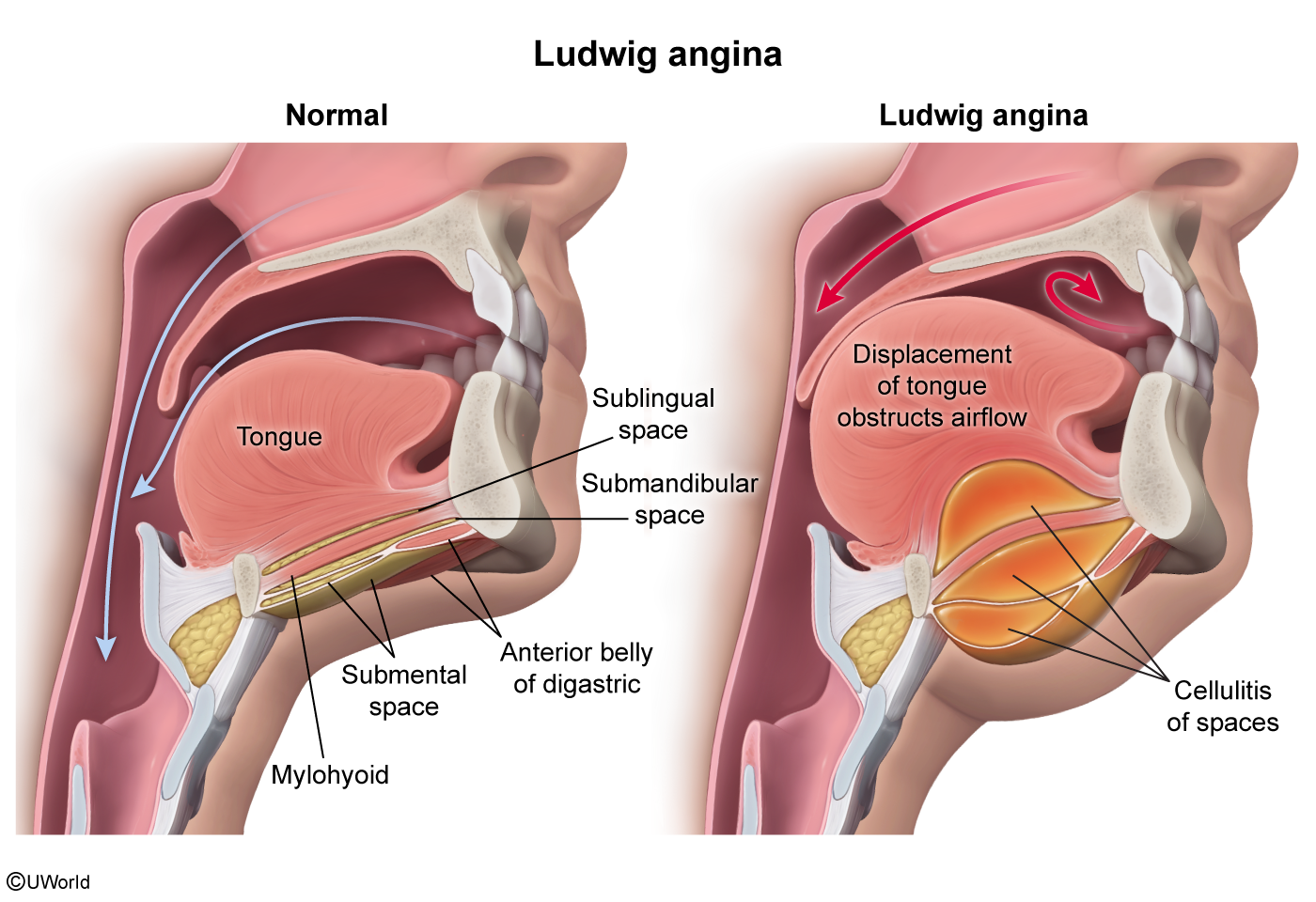
- Presentation: Rapidly progressive, bilateral cellulitis of submandibular, sublingual, and submental spaces.
- Physical Exam:
- “Woody” or brawny, non-fluctuant induration of the submandibular region.
- Elevation and posterior displacement of the tongue (can cause acute airway obstruction).
- Drooling, dysphagia, odynophagia, trismus, muffled (“hot potato”) voice, stridor.
- Systemic signs: Fever, chills, tachycardia.
- Diagnosis
- Initial: Primarily clinical diagnosis. Do NOT delay airway management for imaging if distress is present.
- Imaging (Stable Pts Only): CT neck w/ contrast (reveals soft-tissue swelling, gas, or fluid collections/abscesses requiring drainage).
- Labs: Leukocytosis with left shift, blood cultures.
- Differential Diagnostics
- Peritonsillar Abscess (Quinsy): Diff by unilateral tonsillar swelling, uvular deviation to contralateral side, lack of submandibular “woody” induration.
- Epiglottitis: Diff by lack of submandibular swelling/dental pain; lateral neck X-ray shows “thumbprint sign”; laryngoscopy shows cherry-red epiglottis.
- Retropharyngeal Abscess: Diff by pain with neck extension, widening of prevertebral space on lateral neck X-ray; more common in children.
- Deep Neck Space Infection (e.g., Parapharyngeal): Diff by lateral neck swelling, medial displacement of lateral pharyngeal wall/tonsil.
- Management
- Airway Management (Top Priority):
- High risk of sudden occlusion. Keep airway cart at bedside.
- Secure airway early via fiberoptic nasotracheal intubation (preferred) or surgical airway (cricothyroidotomy/tracheostomy) if intubation fails/impossible due to trismus/swelling.
- IV Antibiotics (Empiric, Broad-Spectrum):
- Ampicillin-sulbactam (Unasyn) OR Ceftriaxone + Metronidazole.
- Add Vancomycin or Linezolid if MRSA suspected (e.g., prior IVDU, dialysis, immunosuppressed).
- Surgical Decompression:
- Urgent incision and drainage (I&D) if purulent collection is present or if medical therapy fails.
- Source Control:
- Extraction of the infected tooth/teeth once stable.
- Complications
- Asphyxiation (most common cause of death).
- Mediastinitis: Spread of infection via the “danger space” (posterior to retropharyngeal space) into the posterior mediastinum.
- Internal Jugular Vein Thrombophlebitis (Lemierre syndrome).
- Sepsis & Septic Shock.