Age of presentation: >60% diagnosed in children <10 yo.
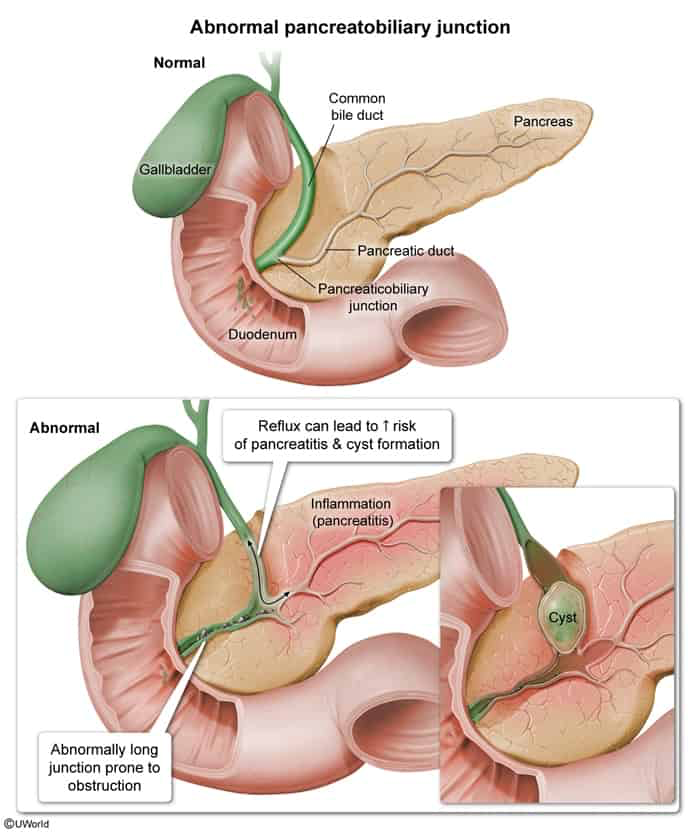
Pathophysiology: Associated with anomalous pancreaticobiliary ductal junction (APBDJ).
Leads to reflux of pancreatic enzymes into biliary tree, causing ductal wall weakening and cyst formation.
Classification: Todani classification (Type I [extrahepatic fusiform dilation of CBD] is most common; Type V is Caroli disease).
Premalignant condition: the entire biliary tree, not just those parts that appear dilated, are at risk of malignant transformation. c
Risk of cholangiocarcinoma is 20–30× higher than in the general population
Clinical Features
Classic Triad (seen in <20% of cases): RUQ pain, jaundice, and a palpable RUQ mass.
Infants: Present with obstructive jaundice, acholic (pale) stools, and hepatomegaly.
Adults: Recurrent RUQ pain, pancreatitis, or cholangitis.
Diagnosis
Initial Test: RUQ Ultrasound (US).
Visualizes cystic structure in the RUQ distinct from the gallbladder.
Confirmatory/Gold Standard Test: MRCP (non-invasive drug of choice for anatomic mapping) or ERCP (invasive, therapeutic if drainage is needed).
Key Labs:
↑ Direct bilirubin, ↑ ALP, ↑ GGT (obstructive jaundice pattern).
↑ Amylase/Lipase (if complicated by pancreatitis).
CBC: leukocytosis (if complicated by cholangitis).
Differential Diagnostics
Biliary Atresia:
Diff by early presentation (<2 months of life) with progressive jaundice, acholic stools, and absent/fibrotic gallbladder on US rather than a distinct cyst. c
Pancreatic Pseudocyst:
Diff by history of pancreatitis, location in the lesser sac, and lack of direct communication with the biliary tree on MRCP.
Gallbladder Duplication:
Diff by two distinct gallbladder lumens with a normal-caliber CBD.
Simple Hepatic Cyst:
Diff by lack of communication with the biliary tree and normal LFTs.
Management
Acute Stabilization (if presenting w/ cholangitis or pancreatitis):
IV fluids, NPO.
Broad-spectrum IV Abx (e.g., Zosyn or Ceftriaxone + Metronidazole).