Pediatric pts: Associated w/ cystic fibrosis (CF) due to chronic coughing/malabsorption straining.
Clinical Features
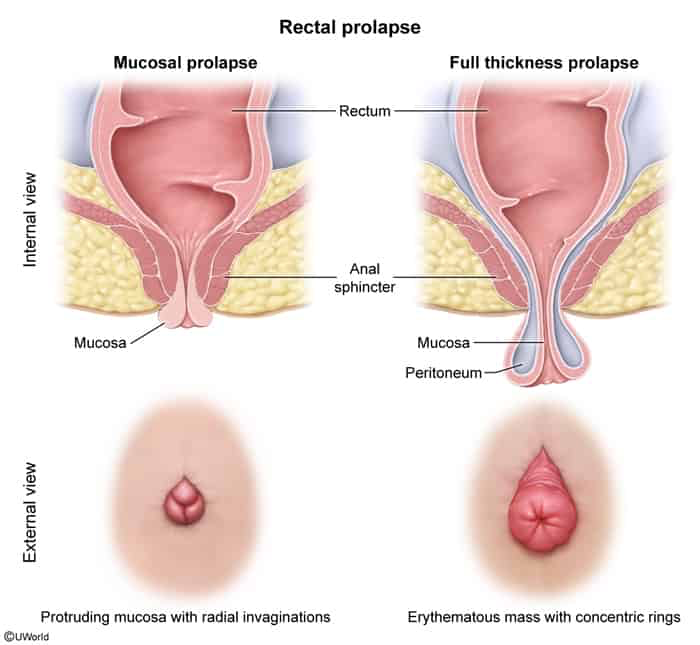
Protruding rectal mass: Red-to-purple mass extending through the anus. c
Inspect for concentric rings of folded rectal mucosa (distinguishes from hemorrhoids).
Mucous discharge and rectal bleeding.
Sensation of incomplete evacuation (tenesmus).
Fecal incontinence (due to chronic sphincter dilation) or constipation.
Diagnosis
Initial: Clinical diagnosis via physical exam. Ask pt to strain/perform valsalva maneuver while seated/squatting to elicit prolapse.
Confirmatory: Clinical inspection of concentric mucosal folds.
Workup:
Sigmoidoscopy/Colonoscopy to rule out underlying rectosigmoid masses/malignancy acting as a lead point.
Defecography if prolapse is suspected but not seen on exam.
Sweat chloride test in pediatric pts w/o clear etiology to rule out CF.
Differential Diagnostics
Prolapsed Internal Hemorrhoids: Diff by presence of radial folds (sulci between hemorrhoidal columns) rather than concentric rings, and lack of full-thickness rectal wall descent.
Rectal Polyp: Diff by presence of a stalk (pedunculated) or a distinct lobulated, localized mass (sessile) rather than circumferential mucosal folds.
Intussusception: Invagination of proximal bowel into distal bowel that does not protrude beyond the anal verge (unless presenting as rectal prolapse, which is a full-thickness intussusception).
Management
Surgical Repair (Definitive for adults):
Abdominal approach (Rectopexy): Preferred for young/fit pts; lower recurrence rate. Rectum is mobilized and fixed to sacral promontory.
Perineal approach (Altemeier or Delorme procedure): Reserved for elderly, frail, or high-operative-risk pts; higher recurrence rate but lower morbidity.