- Anatomical Classification
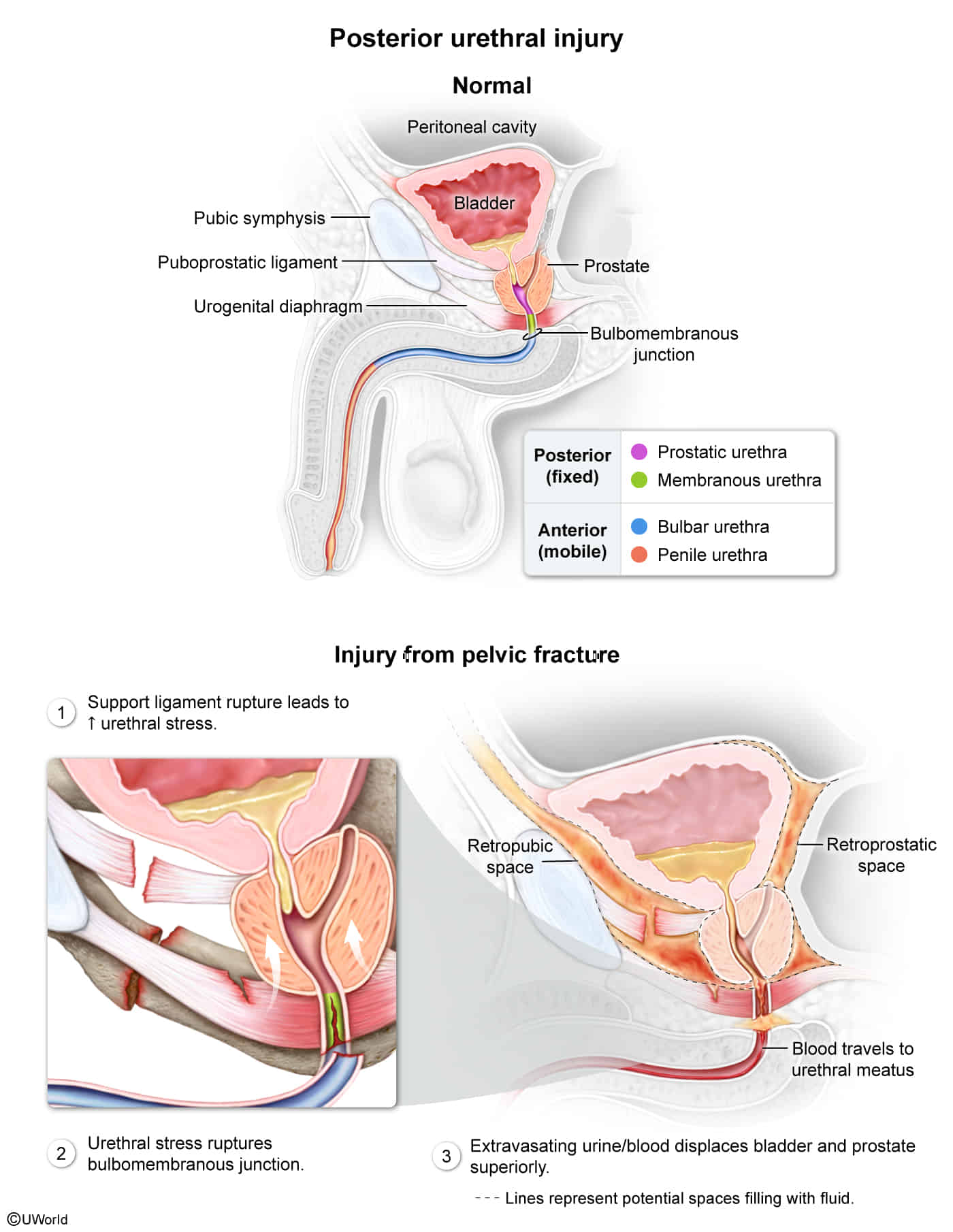
- Posterior Urethra: Membranous (narrowest, most common site of injury) and Prostatic segments.
- Anterior Urethra (Spongy urethra): Bulbar and Penile segments. t
- Etiology
- Posterior Urethral Injury:
- Associated with pelvic fractures (e.g., MVA).
- Shearing force at the prostatomembranous junction.
- Anterior Urethral Injury:
- Associated with straddle injuries (e.g., falling on a bicycle crossbar), direct perineal trauma, or instrumentation t .
- Crushing of the bulbar urethra against the pubic symphysis.
- Clinical Presentation
- General Signs (both anterior & posterior):
- Blood at the urethral meatus (most common and reliable sign).
- Inability to void/urinate.
- Distended bladder (palpable suprapubic mass).
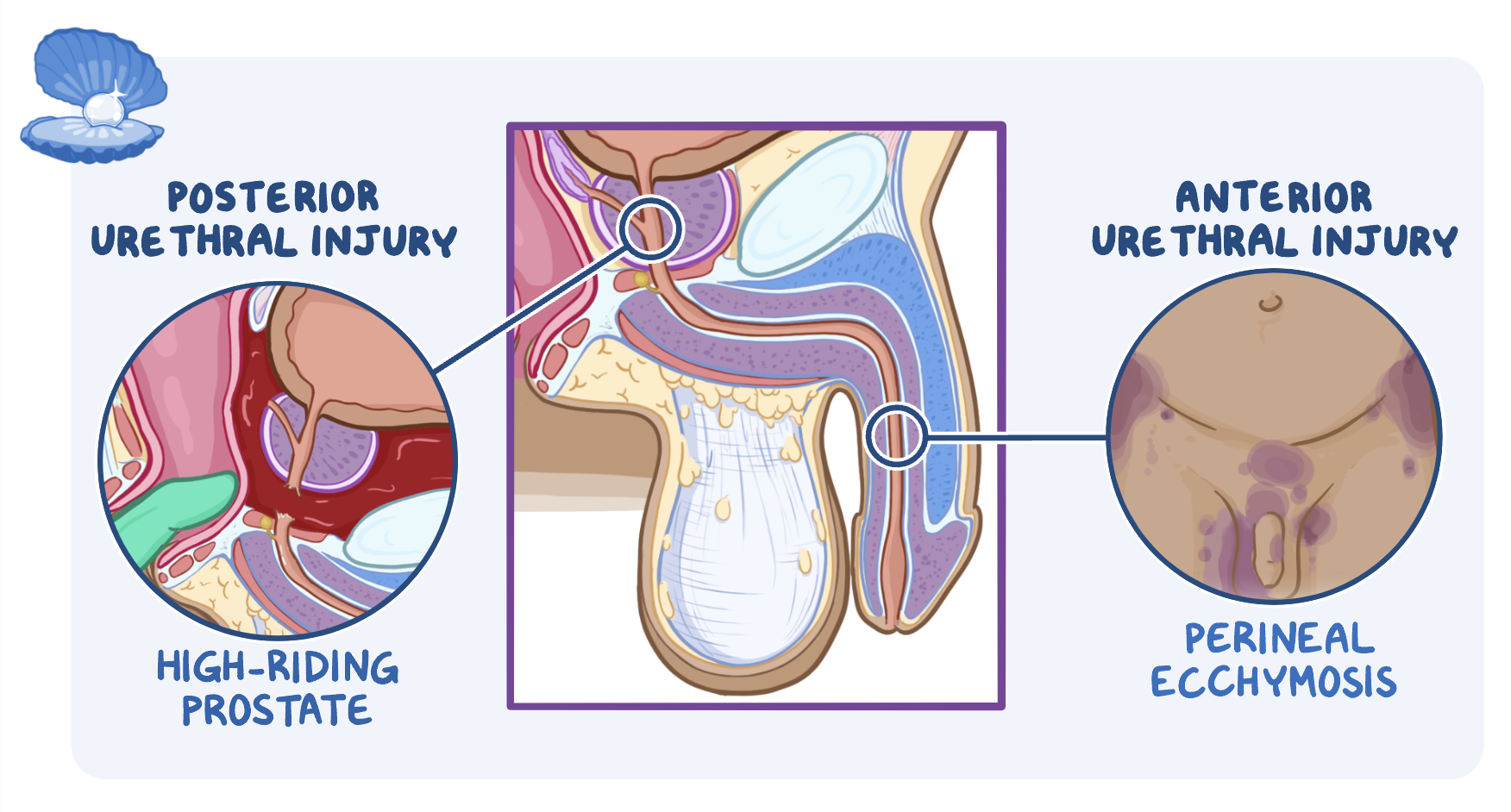
- Posterior Urethral Injury Specifics:
- High-riding prostate on digital rectal exam (DRE) due to disruption of puboprostatic ligaments (poor sensitivity but highly tested). c
- Also, the expanding pelvic hematoma physically pushes the detached bladder and prostate superiorly (cranially) into the pelvis
- Pelvic instability/pain.
- Anterior Urethral Injury Specifics:
- Normal prostate on DRE.
- “Butterfly” hematoma of the perineum, scrotum, and penis (extravasation of blood/urine limited by Colles’ fascia).
- Diagnostics
- Initial & Gold Standard: Retrograde urethrogram (RUG). c
- Contrast injected into the distal urethra; extravasation of contrast confirms the tear (partial vs. complete).
- Key Contraindication: Do NOT insert a Foley catheter before performing RUG if a urethral injury is suspected. c
- Risk of converting a partial urethral tear into a complete transection and introducing infection.
- Key Labs: Urinalysis (usually gross hematuria, though RUG is prioritized over UA).
- Management
- Immediate Urinary Diversion (First-line):
- Place a suprapubic catheter to decompress the bladder and divert urine away from the injured area.
- Safe to perform when the bladder is palpable/distended.
- Surgical Intervention (Second-line/Definitive):
- Delayed urethral reconstruction (urethroplasty) typically performed 3–6 months later after pelvic hematoma and inflammation resolve.
- Immediate primary endoscopic realignment may be considered in select stable patients.
- Refractory/Late Stricture Management:
- Endoscopic dilation or direct vision internal urethrotomy (DVIU) for short, focal strictures.