Epidemiology
Most common cause of nephrotic syndrome in adults, especially in African American and Hispanic populations
Etiology
- Most common cause of nephrotic syndrome in US adults (especially African Americans).
- Primary (Idiopathic): Associated with APOL1 gene mutations in African descent.
- Secondary causes:
- HIV infection (collapsing variant - highly aggressive).
- Heroin use.
- Morbid obesity. c
- Sickle cell disease.
- Pamidronate/Interferon therapy.
- Adaptive hyperfiltration (e.g., unilateral renal agenesis).
Pathophysiology
Injury to podocytes leads to effacement of foot processes and subsequent sclerosis and hyalinosis.
Clinical features
Diagnostics
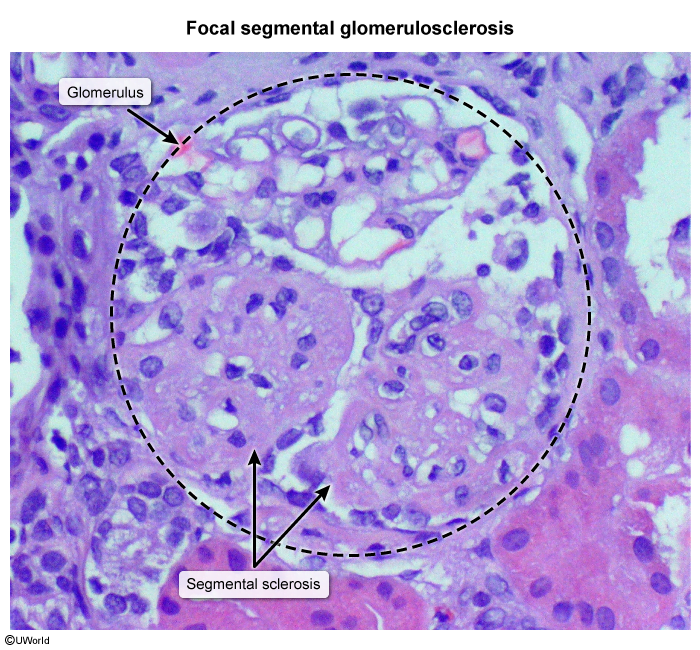
- LM: segmental sclerosis and hyalinosis
- EM: effacement of podocyte foot processes (similar to minimal change disease)
Treatment
- Symptomatic & Supportive (All patients):
- ACE inhibitors (ACEi) or ARBs to reduce intraglomerular pressure and proteinuria.
- Loop diuretics (e.g., Furosemide) for edema control.
- Statins for hyperlipidemia.
- Sodium restriction (< 2 g/day).
- First-line Immunosuppression (Primary FSGS):
- Oral Corticosteroids (prednisone 1 mg/kg/day) for prolonged course (minimum 4-6 months; slower response than MCD).
- Second-line / Steroid-resistant:
- Calcineurin inhibitors (Cyclosporine or Tacrolimus).
- Secondary FSGS:
- Treat underlying cause (e.g., HAART for HIV, weight loss for obesity, discontinue heroin/offending drugs). Do not use immunosuppressants for secondary FSGS. c