Underlying Pathophysiology
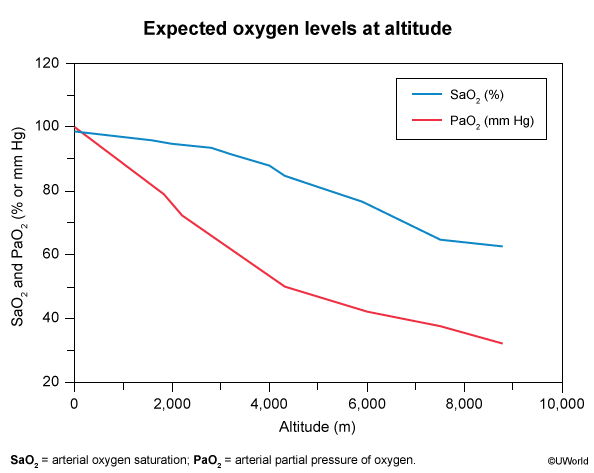
Hypobaric hypoxia : ↓ barometric pressure at high altitude → ↓ partial pressure of inspired O2 (PiO2) → ↓ arterial O2 saturation (SaO2).The primary insult is hypoxia. Illnesses result from failed or incomplete acclimatization.
Physiologic Acclimatization
Immediate (minutes to hours) :
Hyperventilation : Hypoxia stimulates peripheral chemoreceptors → ↑ respiratory rate → respiratory alkalosis.↑ Sympathetic activity: Tachycardia, ↑ cardiac output.
Intermediate (days) :
↑ 2,3-BPG : Right-shifts the O2-hemoglobin dissociation curve, facilitating O2 unloading to tissues.Renal compensation : ↑ HCO3⁻ excretion to correct respiratory alkalosis.
Long-term (weeks to months) :
↑ Erythropoietin (EPO) : Secreted by kidneys in response to hypoxia → ↑ hematocrit and hemoglobin concentration.
Prophylaxis
Primary method : Gradual ascent (allows for acclimatization).Pharmacologic : Acetazolamide . c
Mechanism: Carbonic anhydrase inhibitor. Causes metabolic acidosis by promoting renal HCO3⁻ excretion. This acidosis offsets respiratory alkalosis and stimulates ventilation.
Started 24-48 hours before ascent.
Spectrum of High-Altitude Illnesses
Acute Mountain Sickness (AMS)
Pathophysiology : Mild cerebral edema. Hypoxia → cerebral vasodilation → ↑ capillary pressure → fluid leak.Clinical Features : Occurs >6-12 hours after ascent.
Headache is the hallmark symptom.PLUS ≥1 of the following: fatigue/weakness, dizziness, nausea/vomiting, anorexia, sleep disturbance.
Treatment :
Halt ascent . Descend if symptoms worsen.Symptomatic Tx: NSAIDs (for headache), antiemetics.
Acetazolamide can be used for treatment as well as prophylaxis.
High-Altitude Cerebral Edema (HACE)
Pathophysiology : Severe, life-threatening progression of AMS. Worsening vasogenic cerebral edema.Clinical Features :
AMS symptoms PLUS neurologic dysfunction.
Ataxia (key finding; difficulty with heel-to-toe walk).Confusion, altered mental status, drowsiness, progressing to coma.
Treatment :
IMMEDIATE DESCENT is life-saving.Dexamethasone : Potent anti-inflammatory, reduces vasogenic edema.Supplemental O2.
High-Altitude Pulmonary Edema (HAPE)
Pathophysiology : Most lethal form. Non-cardiogenic pulmonary edema.
Hypoxia → uneven pulmonary vasoconstriction → ↑ pulmonary artery pressure → endothelial damage → alveolar fluid leakage.
Clinical Features
Early: dyspnea on exertion → dyspnea at rest, dry cough, ↓ exercise tolerance.
Late: pink/frothy sputum, cyanosis, tachypnea, tachycardia, low-grade fever .
Compared to pneumonia , HAPE may also present with a low-grade fever and leukocytosis. However, unlike pneumonia, HAPE symptoms typically resolve rapidly within a few hours following supplemental O2 treatment. c
PE: crackles/rales (often R mid-lung first), ↓ SpO₂ out of proportion to altitude.
May coexist with AMS (HA, N/V) or HACE (ataxia, AMS, encephalopathy).
Treatment :
IMMEDIATE DESCENT .Supplemental O2.
Pharmacologic Tx to ↓ pulmonary artery pressure:
Nifedipine (calcium channel blocker).Sildenafil/Tadalafil (phosphodiesterase-5 inhibitors).