Syndrome Bilirubin Type Defect Key Differentiator(s) Gilbert Unconjugated ↓ UGT1A1 Activity Benign; jaundice with stress. ; onset on puberty Crigler-Najjar I Unconjugated Absent UGT1A1Severe; kernicterus risk; no response to phenobarbital. Crigler-Najjar II Unconjugated <20% UGT1A1Less severe; responds to phenobarbital. Dubin-Johnson Conjugated MRP2 Excretion Defect Benign; black liver . Rotor Conjugated OATP Uptake Defect Benign; normal liver color .
Gilbert Syndrome (GS)
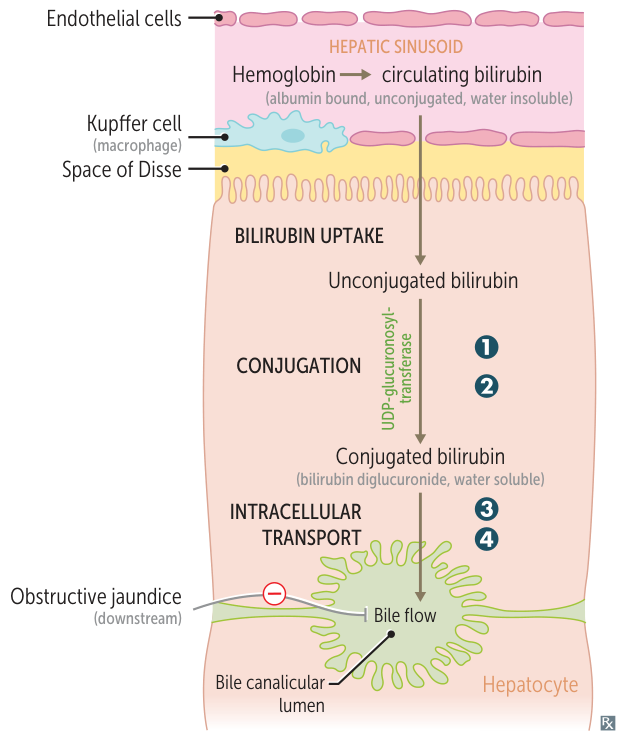
Etiology : Common AR promoter mutation (A(TA)7TAA) leading to mildly decreased UGT1A1 activity (~30% of normal).Clinical Features :
Asymptomatic or mild, transient jaundice triggered by stress, fasting, dehydration, illness, physical exertion, or menstruation . c
Often diagnosed incidentally during routine labs in young adults.
Diagnosis :
Isolated unconjugated hyperbilirubinemia (typically <3 mg/dL ).Normal LFTs and CBC (no hemolysis).
Management :
Reassurance only; benign condition with normal life expectancy. No Tx indicated.
Dubin-Johnson Syndrome
Diagnostics
Initial Labs : Isolated conjugated (direct) hyperbilirubinemia .
Normal AST, ALT, ALP, GGT, and bile acids.
Urine Coproporphyrin : Normal total coproporphyrin, but coproporphyrin I is >80% (normal is coproporphyrin III predominance).Liver Biopsy (rarely indicated, highly diagnostic): Grossly black/dark liver due to accumulation of epinephrine metabolites (coarse pigment in lysosomes). c Imaging : Gallbladder is not visualized on oral cholecystography.