Epidemiology
Etiology
- Pathogen: Plasmodia
- P. falciparum: Most severe; irregular fever patterns; occludes capillaries (parasitized RBCs adhere to endothelium).
- Plasmodium vivax and Plasmodium ovale only infect reticulocytes. In contrast, Plasmodium falciparum has the unique ability to infect erythrocytes of all ages. That’s why it has irregular fever.
- No hypnozoites; recrudescence may occur due to treatment failure, not true relapse.
- Can make RBCs adhere to endothelium, causing occlusions.
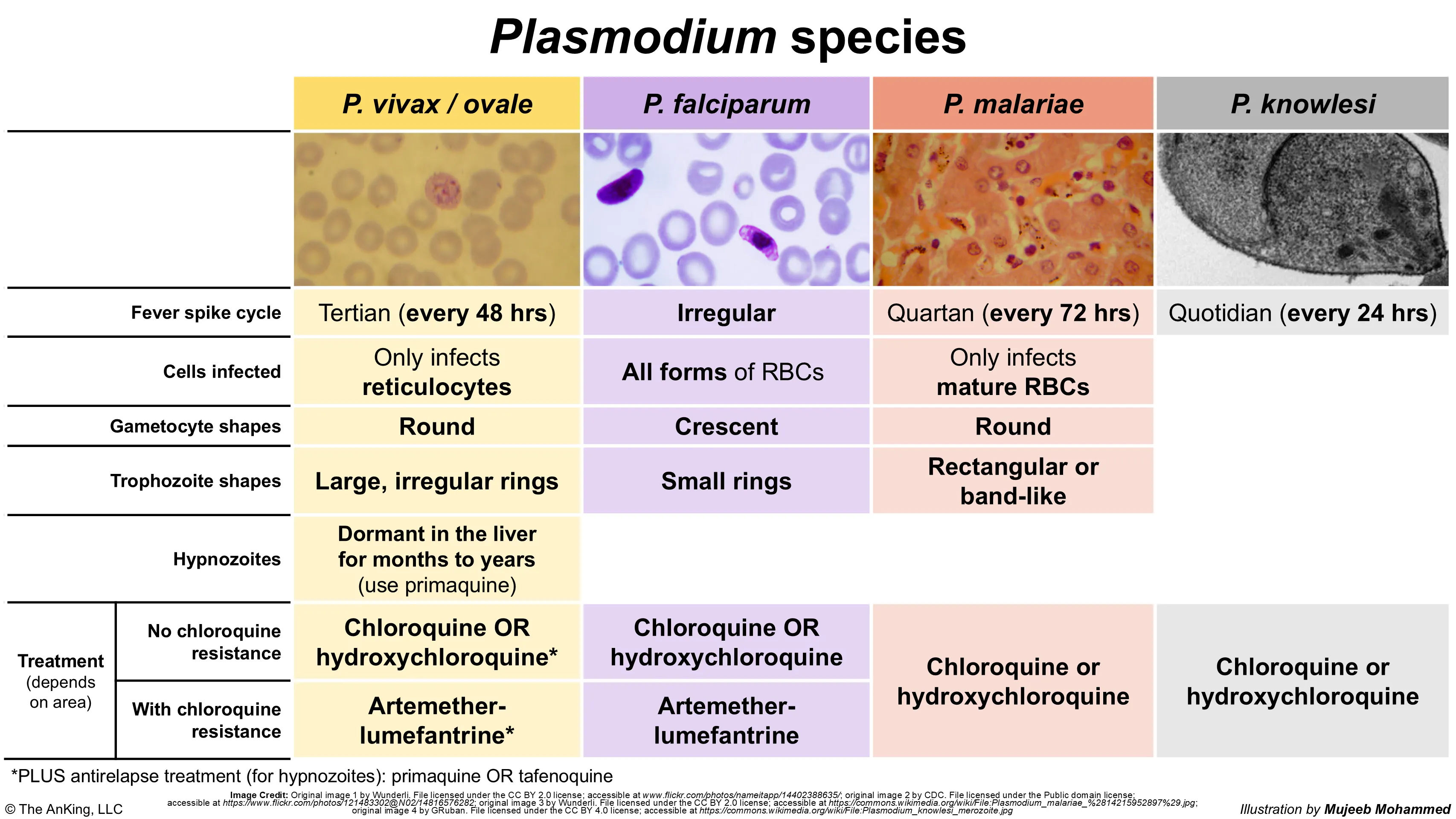
- P. vivax / P. ovale: 48-hr cycle (tertian); dormant form (hypnozoites) in liver cause relapse.
- P. malariae: 72-hr cycle (quartan).
- P. falciparum: Most severe; irregular fever patterns; occludes capillaries (parasitized RBCs adhere to endothelium).
| Feature | P. falciparum | P. vivax / P. ovale | P. malariae | P. knowlesi |
|---|---|---|---|---|
| Fever | Irregular | 48 hrs (Tertian) | 72 hrs (Quartan) | 24 hrs (Quotidian) |
| Smear | Banana gametocyte Headphone rings | Schüffner dots Enlarged RBCs | Band forms Rosettes | Resembles P. malariae |
| Hepatic Dormancy | No | Yes (Hypnozoites), can cause relapse months/years later | No | No |
| Key Note | Severe (Cerebral, Renal) Occludes capillaries | Vivax: No infection if Duffy (-) | Nephrotic syndrome | Zoonotic (Macaques) SE Asia |
| Tx | ACT (Artemether) Chloroquine-Resistant | Add Primaquine (Check G6PD) | Chloroquine | Same as P. falciparum |
Pathophysiology
Asexual development in humans
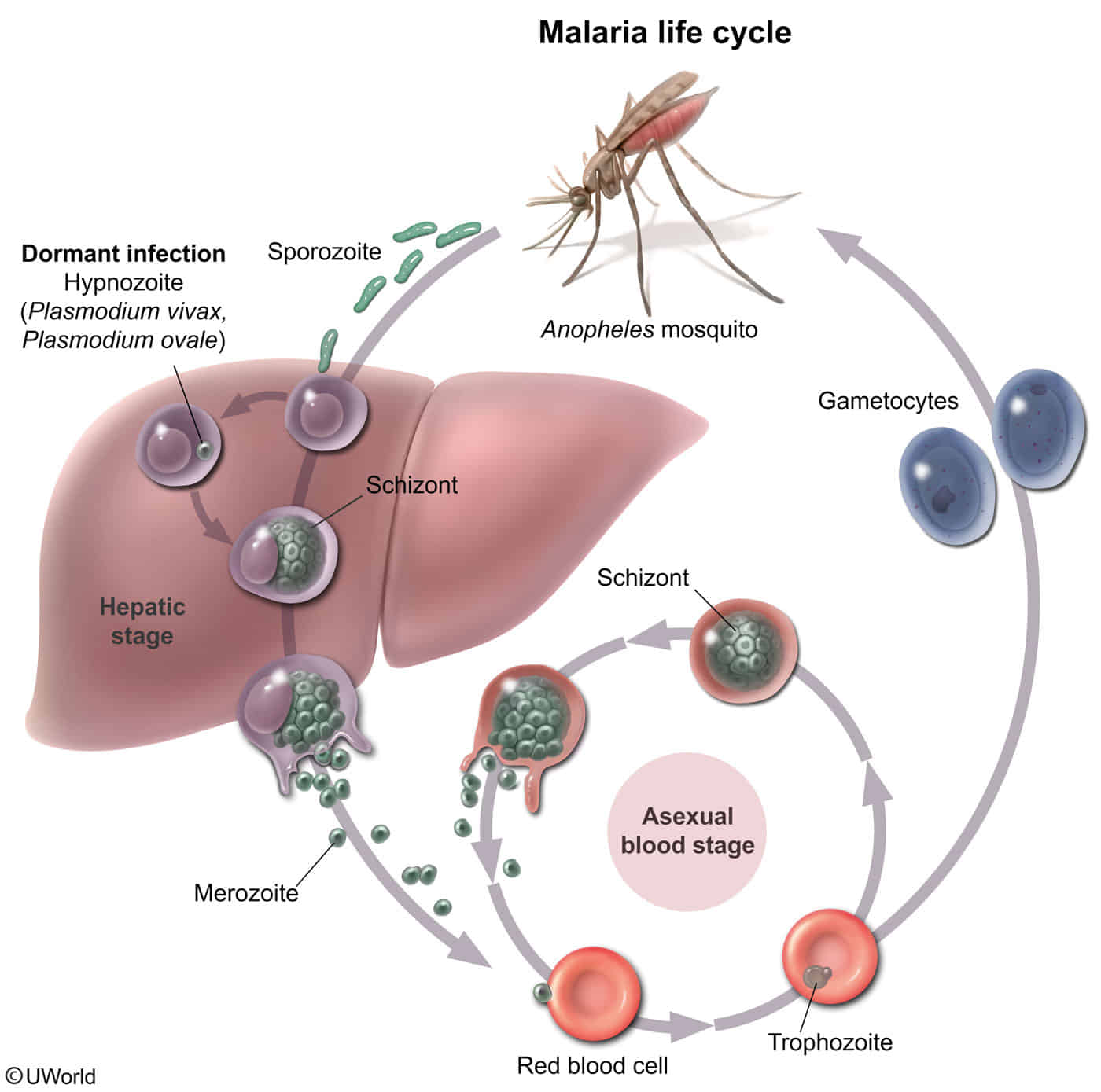
- Transmission of Plasmodium sporozoites via Anopheles mosquito bite → sporozoites travel through the bloodstream to the liver of the host
- Liver: sporozoites enter hepatocytes → sporozoites multiply asexually → schizonts are formed containing thousands of merozoites → release of merozoites into the bloodstream
- Circulatory system (two possible outcomes)
- Merozoites enter erythrocytes → maturation to trophozoites → red cell schizonts are formed containing thousands of merozoites → release of merozoites into the bloodstream (which causes fever and other manifestations of malaria) → penetration of erythrocytes recurs
- Merozoites enter erythrocytes → differentiation into gametocytes (male or female)
- Following the successful treatment of tertian malaria, dormant P. ovale or P. vivax forms (hypnozoites) may remain in the liver and can cause relapse after months or even years.
Clinical features
Diagnostics
- Blood Smear (Gold Standard):
- Thick smear: Detects presence of parasites (screening).
- Thin smear: Identifies species.
- Key Findings:
- P. falciparum: Banana-shaped gametocytes, headphone-shaped ring forms, multiple rings per RBC.
- P. vivax/ovale: Schüffner stippling (red granules in RBC cytoplasm), enlarged RBCs.
- P. malariae: Band forms.
- P. knowlesi: PCR often needed to distinguish; infects macaques.
Treatment
- Chloroquine-sensitive regions: Chloroquine (blocks heme polymerase).
- Chloroquine-resistant P. falciparum:
- Artemisinin-based combination therapy (ACT) (e.g., Artemether-Lumefantrine).
- Atovaquone-Proguanil.
- Severe Malaria: IV Artesunate (preferred) or IV Quinidine (monitor for QT prolongation/hypoglycemia).
- P. vivax / P. ovale (Hypnozoites): Add Primaquine or Tafenoquine to kill liver phase.
- High-Yield: MUST check for G6PD deficiency before giving Primaquine (risk of severe hemolysis).
Antimalarial drugs
- Primaquine is the only antimalarial that attacks the hypnozoites, preventing relapse
- Chloroquine:
- MOA: Blocks heme detoxification.
- Use: Tx of sensitive malaria; Prophylaxis in sensitive areas.
- SE/CI: Pruritus, retinopathy (chronic use). Widespread P. falciparum resistance. Safe in pregnancy.
- Primaquine / Tafenoquine:
- MOA: Kills liver hypnozoites (disrupts mitochondrial e- transport).
- Use: Radical cure for P. vivax & P. ovale. Terminal prophylaxis (P. vivax).
- SE/CI: Hemolytic anemia in G6PD deficiency (MUST TEST!). Contraindicated in pregnancy, G6PD deficiency.
- Artemisinins (IV Artesunate, Artemether-Lumefantrine):
- MOA: Free radical damage (via endoperoxide bridge activation by heme). Rapid acting.
- Use: IV Artesunate = 1st line for SEVERE P. falciparum. Artemisinin Combination Therapies (ACTs) = 1st line for uncomplicated chloroquine-resistant P. falciparum.
- SE/CI: Generally well-tolerated. ACTs preferred. Artemether-lumefantrine often used in pregnancy.
- Atovaquone-Proguanil (Malarone):
- MOA: Atovaquone (mito e- transport inhibitor) + Proguanil (DHFR inhibitor).
- Use: Prophylaxis & Tx of chloroquine-resistant P. falciparum.
- SE/CI: GI upset (take with food). Contraindicated: severe renal impairment, pregnancy (generally).
- Mefloquine:
- MOA: Unclear (likely heme polymerization inhibitor).
- Use: Prophylaxis (weekly) & Tx of chloroquine-resistant P. falciparum.
- SE/CI: Neuropsychiatric effects (BLACK BOX WARNING!) - vivid dreams, psychosis, seizures. Contraindicated: psychiatric disorders, seizures. Use with caution in pregnancy.
- Quinine / Quinidine (IV):
- MOA: Unclear (likely heme polymerization inhibitor).
- Use: Tx chloroquine-resistant P. falciparum (often + doxycycline/clindamycin). IV Quinidine for severe malaria if artesunate unavailable.
- SE/CI: Cinchonism (tinnitus, headache, dizziness), hypoglycemia, QTc prolongation.
- Doxycycline:
- MOA: 30S ribosomal inhibitor.
- Use: Prophylaxis (daily) for resistant malaria. Tx (with quinine) for resistant P. falciparum.
- SE/CI: Photosensitivity, GI upset (esophagitis). Contraindicated: pregnancy, children <8 years.
- Clindamycin:
- MOA: 50S ribosomal inhibitor.
- Use: With quinine for resistant P. falciparum (esp. pregnancy 1st trimester as alternative).
- SE/CI: Diarrhea, C. difficile colitis.
Plans
- Chloroquine-Resistant P. falciparum:
- Uncomplicated: ACTs (e.g., Artemether-Lumefantrine) = First line.
- Severe: IV Artesunate = First line. (IV Quinidine + Doxycycline if artesunate unavailable).
- P. vivax / P. ovale (Relapsing Malaria): Treat blood stages (e.g., chloroquine if sensitive, or ACT) PLUS Primaquine or Tafenoquine for liver hypnozoites (radical cure – check G6PD status!).
- Prophylaxis (Chloroquine-Resistant Areas): Atovaquone-Proguanil, Doxycycline, or Mefloquine.
- Pregnancy:
- Uncomplicated P. falciparum: Artemether-lumefantrine preferred. Quinine + Clindamycin (esp. 1st trimester).
- Severe: IV Artesunate.
- Contraindicated: Doxycycline, Primaquine, Tafenoquine. Atovaquone-Proguanil generally avoided.
- G6PD Deficiency: NO Primaquine or Tafenoquine. Use Quinine with caution.
Prevention
- Atovaquone-Proguanil: Daily, good for last-minute travelers.
- Mefloquine: Weekly; neuropsychiatric side effects (avoid in pts with psych Hx or seizures).
- Doxycycline: Daily; photosensitivity, teratogenic.
- Chloroquine: Only for sensitive zones, maybe ineffective t (Caribbean, parts of Central America).
Tip
Prophylactic medication cannot prevent infection but instead suppresses the course of the disease and its symptoms by killing the parasite within the host before it can cause severe disease. There is no prophylactic medication that provides protection against all species of the Plasmodium genus.