Epidemiology
Etiology
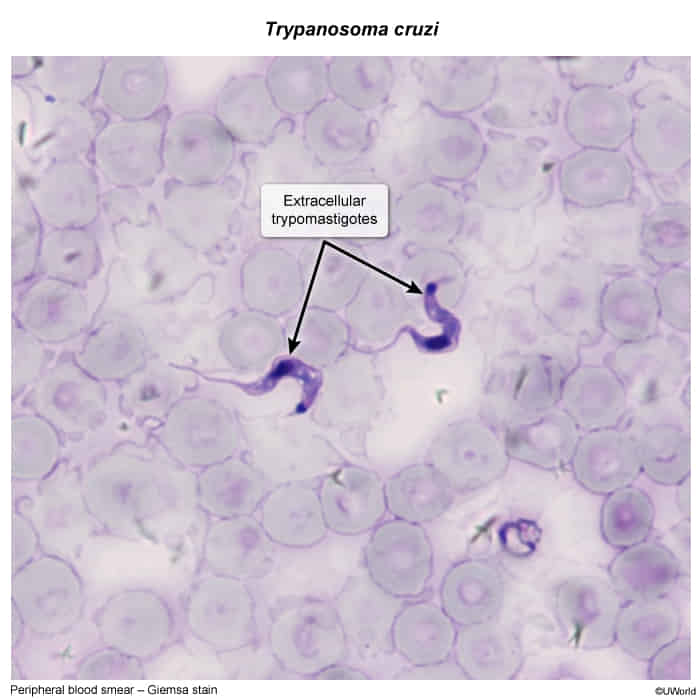
- Pathogen: Trypanosoma cruzi
- Route of infections
- Vector transmission
- Numerous triatomine species of the Reduviidae family (also called kissing bug because it typically bites around the mouth)
- They hide in the cracks of houses and usually bite individuals in their sleep.
- T. cruzi is shed in the feces of the reduviid bug; feces is then rubbed into the bite site while scratching.
- Numerous triatomine species of the Reduviidae family (also called kissing bug because it typically bites around the mouth)
- Vector transmission
Pathophysiology
Clinical features
- Acute Phase (< 2 months):
- Mostly asymptomatic or mild viral-like illness.
- Romaña sign: Unilateral painless periorbital edema (site of conjunctival inoculation).
- Chagoma: Nodular swelling at the bite site.
- Romana sign is seen when the portal of entry of T. cruzi is the conjunctiva. Patients may also present with ipsilateral conjunctivitis and preauricular lymph node enlargement.
- Fever, LAD, HSM. Rarely acute severe myocarditis or meningoencephalitis.
- Chronic Phase (develops years/decades later in ~30% of pts):
- Cardiac: Dilated cardiomyopathy (biventricular HF), LV apical aneurysm (classic buzzword), arrhythmias (ventricular, RBBB, LAFB), mural thrombi.
- GI: Destruction of enteric nervous system (Auerbach plexus).
- Megaesophagus: Secondary achalasia (progressive dysphagia, regurgitation, weight loss).
- Megacolon: Chronic severe constipation, abdominal distension.
Diagnostics
Best initial test: direct visualization of T. cruzi trypomastigotes in thin and thick peripheral blood smears using a Giemsa stain