A condition of bleeding from the biliary tree.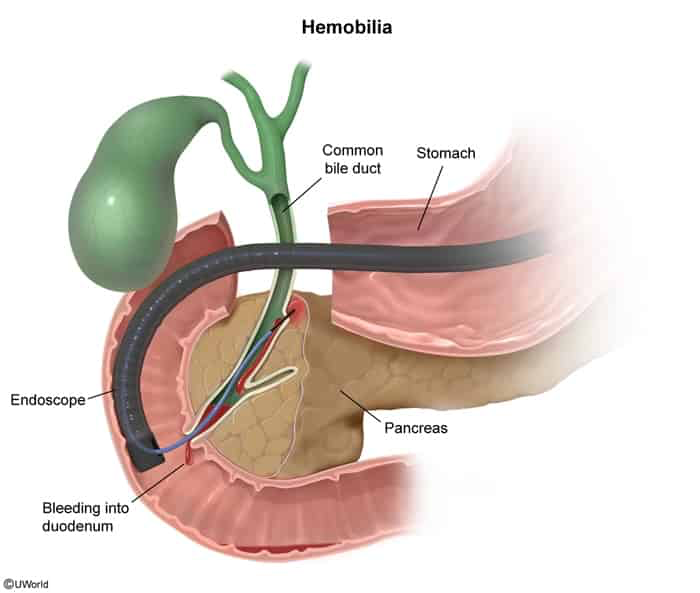
Epidemiology & Risk Factors
- Iatrogenic trauma is the most common cause (>50% of cases): c
- Percutaneous liver biopsy.
- Percutaneous transhepatic cholangiography (PTC) or percutaneous biliary drainage (PTBD).
- ERCP or laparoscopic cholecystectomy.
- TIPS procedure.
- Non-iatrogenic trauma (blunt or penetrating abdominal trauma).
- Vascular abnormalities:
- Hepatic artery pseudoaneurysm or aneurysm rupture.
- Arterio-biliary fistulae.
- Hepatobiliary malignancies (cholangiocarcinoma, hepatocellular carcinoma [HCC], liver metastases).
- Gallstones (eroding into hepatic vessels) and parasitic infections (e.g., Ascaris lumbricoides).
Clinical Features
- Quincke’s Triad (present in ~30–40% of cases):
- RUQ pain (biliary colic due to clot obstruction/distension).
- Obstructive jaundice (from clots blocking bile ducts).
- Upper GI bleeding (melena, hematemesis, or hematochezia).
- History of recent hepatobiliary instrumentation (days to weeks prior).
- Signs of hemorrhagic shock/anemia (tachycardia, hypotension, pallor) in severe hemorrhage.
Diagnosis
- Initial Lab Testing:
- Complete Blood Count (CBC): ↓ Hb/Hct (anemia).
- LFTs: ↑ Direct Bilirubin, ↑ ALP & GGT (obstructive pattern). Mild-to-moderate ↑ AST/ALT.
- Coagulation panel (PT/INR, PTT) to assess for underlying coagulopathy.
- Initial Imaging:
- RUQ Ultrasound: Often the first test. Shows echogenic material (blood clots) in the gallbladder or bile ducts, ductal dilation, or rules out other biliary pathology.
- CT Abdomen / CT Angiography (CTA): Identifies vascular etiologies (e.g., pseudoaneurysms, fistulae), parenchymal hematoma, or active contrast extravasation.
- Confirmatory / Gold Standard:
- Angiography: Most sensitive and specific for identifying vascular lesions (e.g., hepatic artery pseudoaneurysm, active arterial bleeding). Provides simultaneous therapeutic intervention.
- EGD / ERCP: Directly visualizes blood/clots egressing from the ampulla of Vater (confirms active hemobilia).
Differential Diagnostics
- Upper GI Bleeding (Non-biliary):
- Peptic Ulcer Disease (PUD) / Mallory-Weiss Tear / Varices: Diff by lack of Quincke’s triad (no jaundice/biliary colic), and EGD shows direct luminal bleeding (e.g., gastric ulcer) rather than blood from the ampulla.
- Choledocholithiasis:
- Diff by absence of hematemesis/melena/anemia. RUQ US shows a gallstone in the CBD rather than mobile echogenic clots.
- Acute Cholangitis:
- Diff by Charcot’s Triad (fever, RUQ pain, jaundice) without overt GI bleeding, and leukocytosis is typically more prominent. (Note: Hemobilia complicated by clot obstruction can trigger secondary cholangitis).
- Aortoenteric Fistula:
- Diff by history of AAA repair or aortic graft, presenting with “herald bleed” followed by catastrophic GI hemorrhage without biliary symptoms.
Management
- 1st Line (Emergency & Stabilization):
- Hemodynamic Resuscitation: Large-bore IV access, IV crystalloids, packed red blood cells (PRBCs) as needed.
- Correct Coagulopathy: Discontinue anticoagulants, administer Vitamin K, Fresh Frozen Plasma (FFP), or platelets.
- Conservative Management: Indicated for minor/self-limiting hemobilia with close observation and biliary drainage if needed.
- 2nd Line (Definitive Management for Persistent/Major Bleeding):
- Transcatheter Arterial Embolization (TAE): Gold standard/first-line intervention for major or ongoing arterial hemobilia. Achieves hemostasis in up to 95% of cases.
- ERCP / Endoscopic Biliary Drainage: Performed to relieve biliary obstruction, extract clots, and place stents to maintain bile duct patency.
- Refractory (Surgical Intervention):
- Indicated if TAE fails, is unavailable, or if bleeding is from a large hepatic artery aneurysm.
- Includes surgical ligation of the bleeding vessel, cholecystectomy (if bleeding is from gallbladder/hemophilic cholecystitis), or segmental hepatic resection.
Complications
- Obstructive Jaundice: Clots plug the common bile duct (CBD).
- Acute Cholangitis: Biliary stasis from clot obstruction leads to bacterial superinfection.
- Acute Pancreatitis: Blood clots obstructing the pancreatic duct (ampulla of Vater blockage).
- Hemorrhagic Shock: Catastrophic blood loss from major arterial laceration.
- Hemocholecystitis: Blood accumulating in the gallbladder, mimicking acute cholecystitis, with a risk of gallbladder necrosis/perforation.