| Feature | Gastroschisis | Omphalocele | Umbilical Hernia |
|---|---|---|---|
| Location | Paraumbilical (Right) | Midline (Umbilical ring) | Midline (Umbilical ring) |
| Covering | None (Exposed viscera) | Sac (Peritoneum + Amnion) | Skin |
| Associations | None (Isolated) | Trisomies (13, 18, 21), Beckwith-Wiedemann | Congenital Hypothyroidism, Down Syndrome |
| Maternal AFP | Markedly ↑ c | Slightly ↑ | Normal |
| Tx/Outcome | Surgery; Good prognosis | Surgery; Prognosis depends on anomalies | Spontaneous closure (wait until age 2-5) |
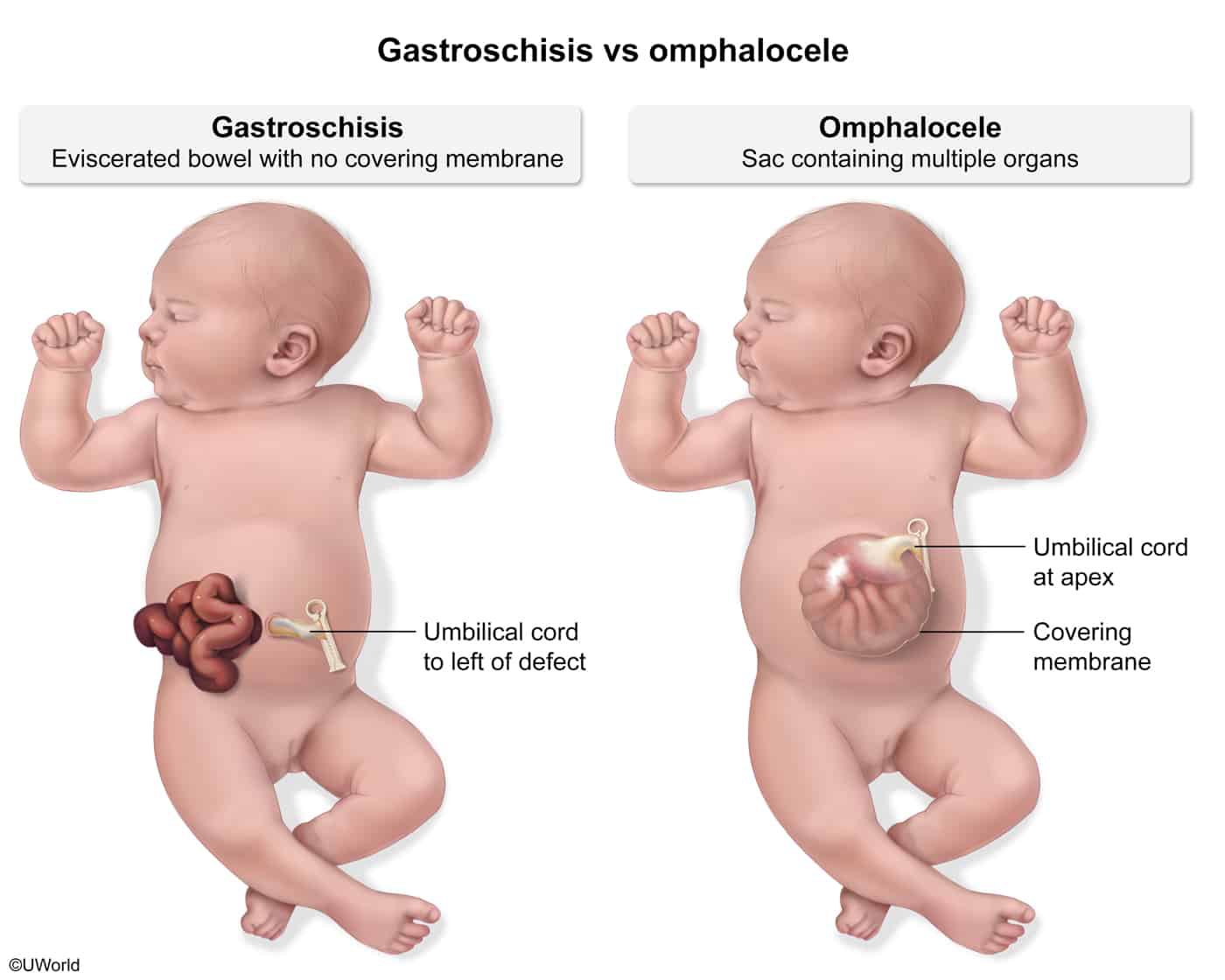
Tip
Unlike in cases of omphalocele, gastroschisis does not manifest with a hernia sac.
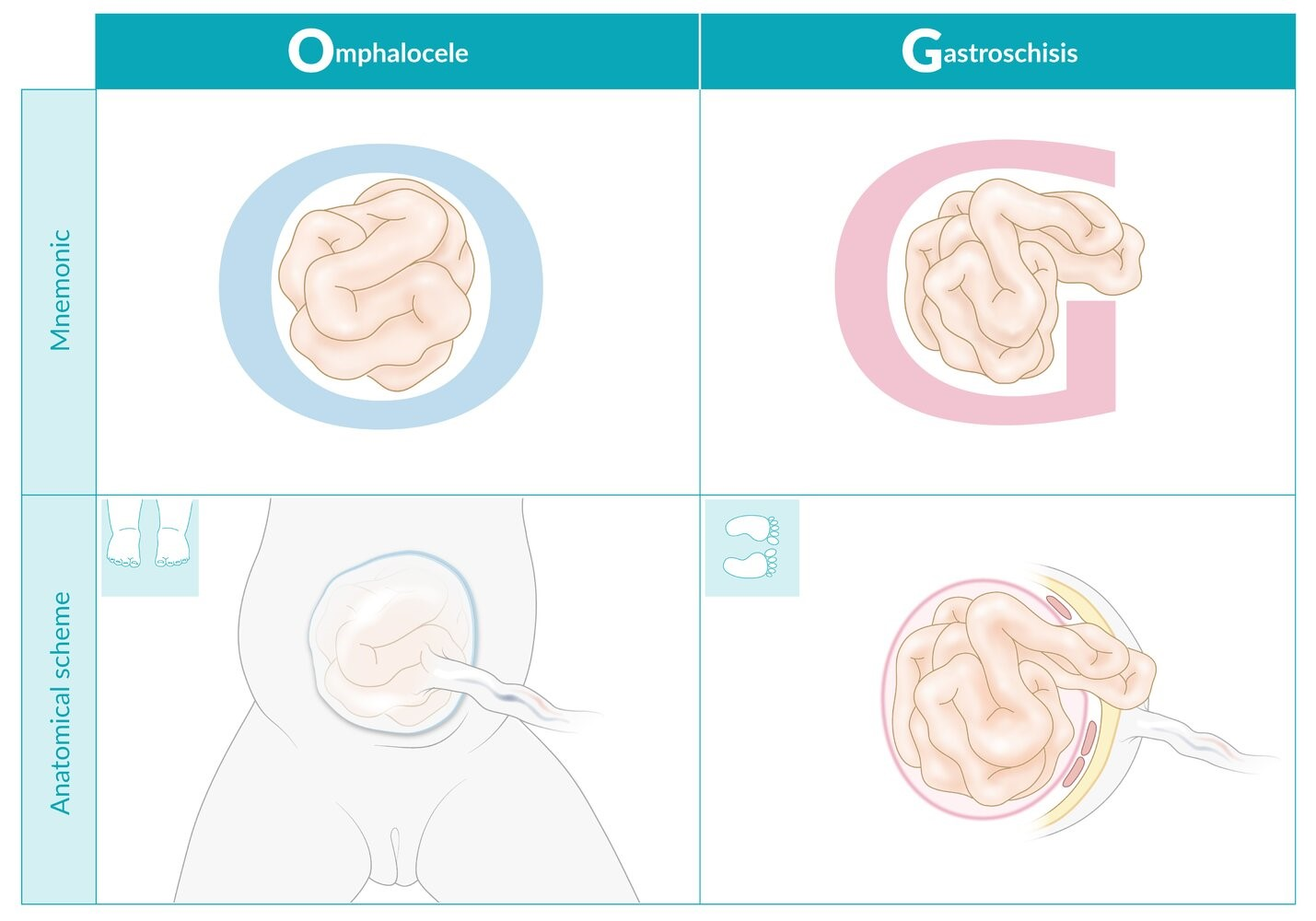
Mnemonic
Omphalocele keeps your gut O-sealed (covered with peritoneum), but in Gastroschisis, the Gut freezes (herniates through the abdominal wall without being covered by peritoneum).
Gastroschisis
Diagnosis
- Initial/Screening: Elevated MSAFP (maternal serum alpha-fetoprotein) in the second trimester (typically higher elevation than in omphalocele).
- Prenatal Imaging: Fetal US showing free-floating, herniated bowel loops in the amniotic cavity (“cauliflower” sign). c
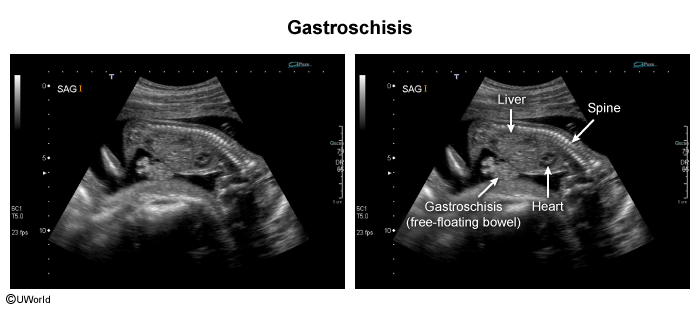
- Confirmatory/Postnatal: Visual inspection on PE at birth.
- Key Labs: No routine genetic testing required as association with karyotypic abnormalities is extremely low.
Congenital Umbilical Hernia
Epidemiology & Risk Factors
- Pathophysiology: Incomplete closure of the umbilical ring (fascial defect).
- Risk Factors:
- Prematurity and low birth weight (LBW).
- African American (AA) infants (up to 10x higher incidence).
- Associated conditions: Down syndrome (Trisomy 21), Beckwith-Wiedemann syndrome, Congenital hypothyroidism, Hurler syndrome.
Clinical Features
- Soft, non-tender, skin-covered protrusion at the umbilicus.
- Protrudes/enlarges with increased intra-abdominal pressure (e.g., crying, coughing, straining).
- Easily reducible through the fascial defect.
- Size ranges from < 1 cm to > 5 cm.
Diagnosis
- Initial & Confirmatory: Clinical diagnosis via physical exam (PE) demonstrating a palpable umbilical fascial defect.
- Imaging (e.g., ultrasound) is not routinely indicated unless incarceration is suspected.
Management
- Observation & Reassurance (First-line):
- Most hernias close spontaneously by age 1-2 years due to growth of rectus abdominis muscles. c
- Reassure parents that taping/strapping (e.g., taping a coin) is ineffective and contraindicated (causes skin irritation/infection).
- Surgical Repair (Elective):
- Indicated if the hernia persists beyond age 5 years.
- Indicated if defect is > 1.5 - 2 cm (unlikely to close spontaneously).
- Indicated if growing rapidly or causing pain.
- Emergency Surgical Repair:
- Indicated immediately if there are signs of incarceration (non-reducible, painful) or strangulation (erythema, warmth, systemic signs).