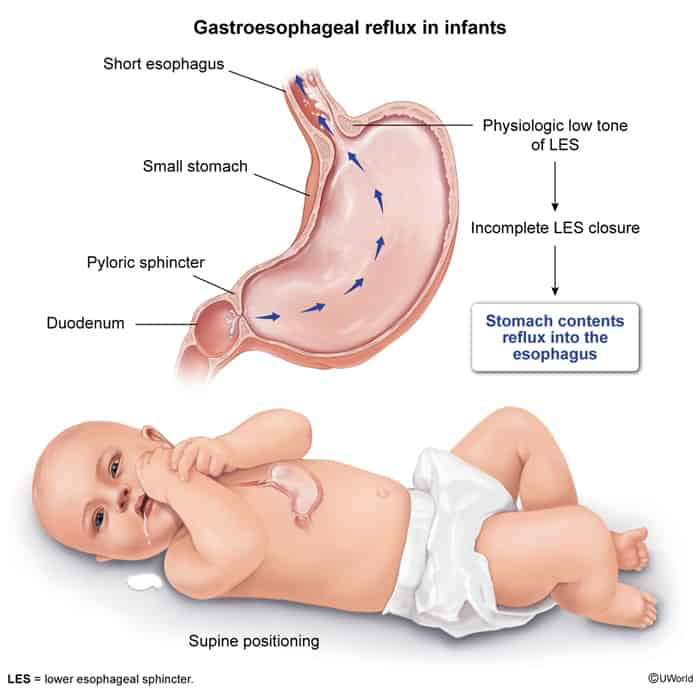
Physiologic GER: Immaturity of the esophageal sphincter mechanism in the first 6 weeks of life. Peak incidence at 4 months; resolves spontaneously by 12–18 months in >90% of infants due to elongation of esophagus and upright posture.
Pathologic GERD: Persistent reflux causing symptoms or complications.
Physiologic GER: Clinical diagnosis based on history and PE. No diagnostic testing required.
Pathologic GERD:
Initial Assessment: Detailed feeding history and growth chart monitoring.
Key Labs: Usually normal; BMP if severe vomiting to rule out metabolic alkalosis.
Diagnostic Trial: 2-to-4-week trial of acid suppression (PPI) in older children with typical symptoms.
Upper GI Series (Barium Swallow): NOT used to diagnose reflux; used to rule out anatomic abnormalities (e.g., malrotation, hiatal hernia, pyloric stenosis).
Confirmatory/Gold Standard (if atypical or refractory):
24-hour pH/Impedance Probe Monitoring: Quantifies acid/non-acid reflux frequency and correlates with symptoms.
Esophagogastroduodenoscopy (EGD) with biopsy: Evaluates for reflux esophagitis, strictures, or Eosinophilic Esophagitis (EoE).
Differential Diagnostics
Pyloric Stenosis:
Diff: Presents at 3–6 weeks of age with progressive, projectile, non-bilious vomiting, hypokalemic hypochloremic metabolic alkalosis, and an “olive-shaped” abdominal mass. Diagnosis confirmed by abdominal US.
Malrotation with Midgut Volvulus:
Diff: Presents with bilious vomiting and acute abdomen. Diagnosis confirmed by Upper GI series showing “corkscrew” duodenum.
Eosinophilic Esophagitis (EoE):
Diff: Pt with history of atopy/allergies presenting with dysphagia or feeding refusal. EGD biopsy shows ≥15 eosinophils/HPF and esophageal trachealization (concentric rings).
Cow’s Milk Protein Allergy (CMPA):
Diff: Presents with vomiting, poor weight gain, and painless hematochezia (blood-streaked stools) or eczema. Diagnosed clinically via maternal dietary elimination (if breastfed) or switching to hydrolyzed formula.
Management
Physiologic GER (“Happy Spitter”):
First-line: Reassurance and education.
Conservative measures:
Avoid overfeeding (smaller, more frequent feeds). c
Keep infant upright for 20–30 minutes post-feed.
Thicken feeds with oatmeal cereal (1 tbsp per oz of formula).
Pathologic GERD:
First-line (Infants):
Two-week trial of hypoallergenic formula (extensively hydrolyzed) or maternal dairy elimination to rule out CMPA.
If no improvement, initiate medical therapy.
First-line (Older Children / Refractory Infants):
Acid suppression: Proton Pump Inhibitors (PPIs) (e.g., omeprazole) or H2 Receptor Antagonists (H2RAs) (e.g., famotidine) for a 4–8 week trial.
Refractory/Severe Cases:
Surgical intervention: Nissen fundoplication reserved for pts with severe GERD refractory to medical therapy, life-threatening complications (e.g., recurrent apnea, severe aspiration), or severe neurologic impairment.
Complications
Esophagitis, esophageal stricture, or Barrett’s esophagus (rare in children).
Failure to thrive (FTT) due to caloric loss/feeding aversion.
Recurrent aspiration pneumonia and chronic airway disease.
Brief Resolved Unexplained Events (BRUE) or apnea.