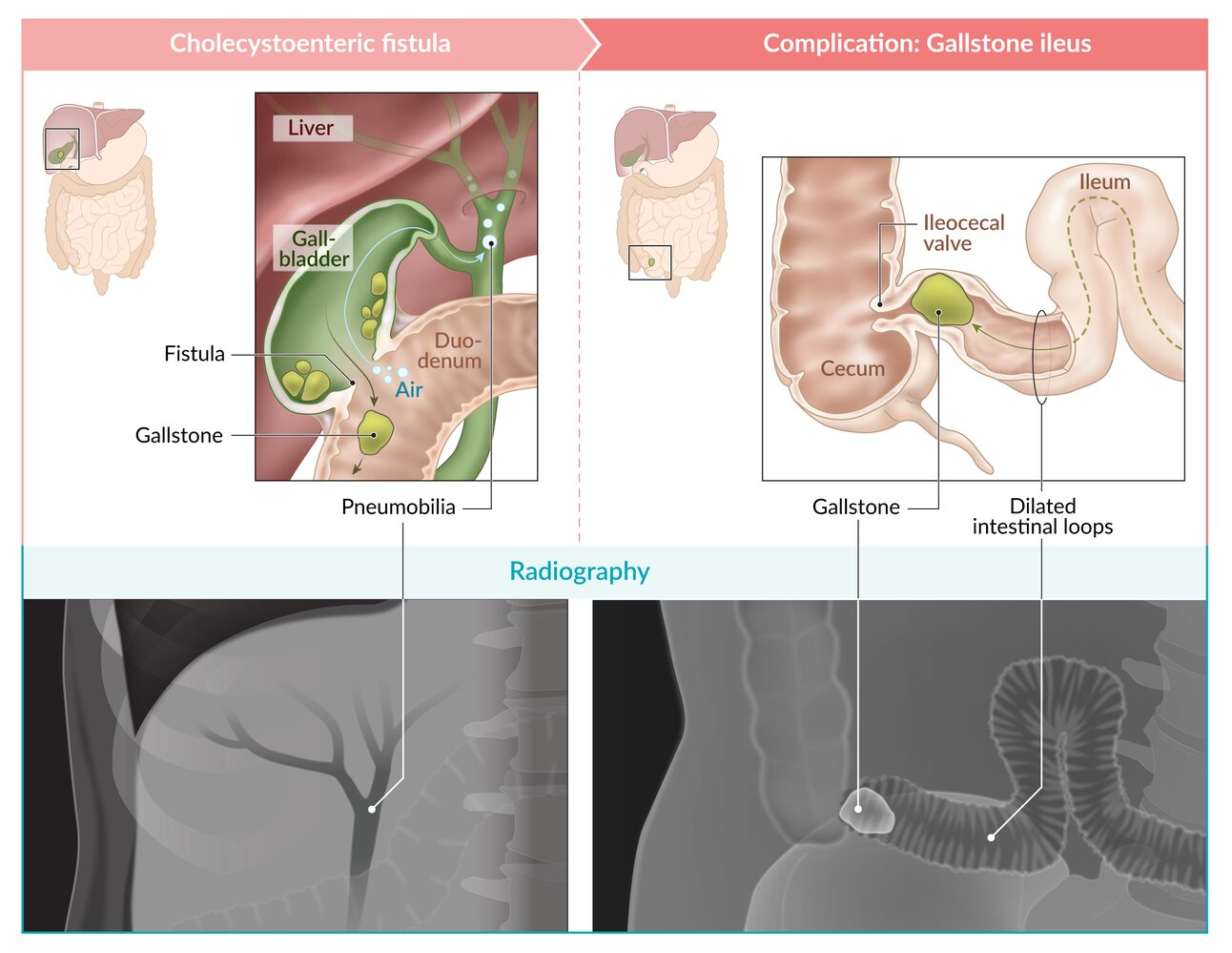
Pathophysiology: gallbladder perforation or Mirizzi syndrome → biliary-enteric fistula formation (most commonly cholecystoenteric fistula) between the inflamed gallbladder and bowel → Gallstones passing down into bowel lumen
Sites of obstruction: terminal ileum, at ileocecal valve (most common)
Symptoms: distal bowel obstruction: features of mechanical bowel obstruction (abdominal pain and distention, nausea, vomiting)
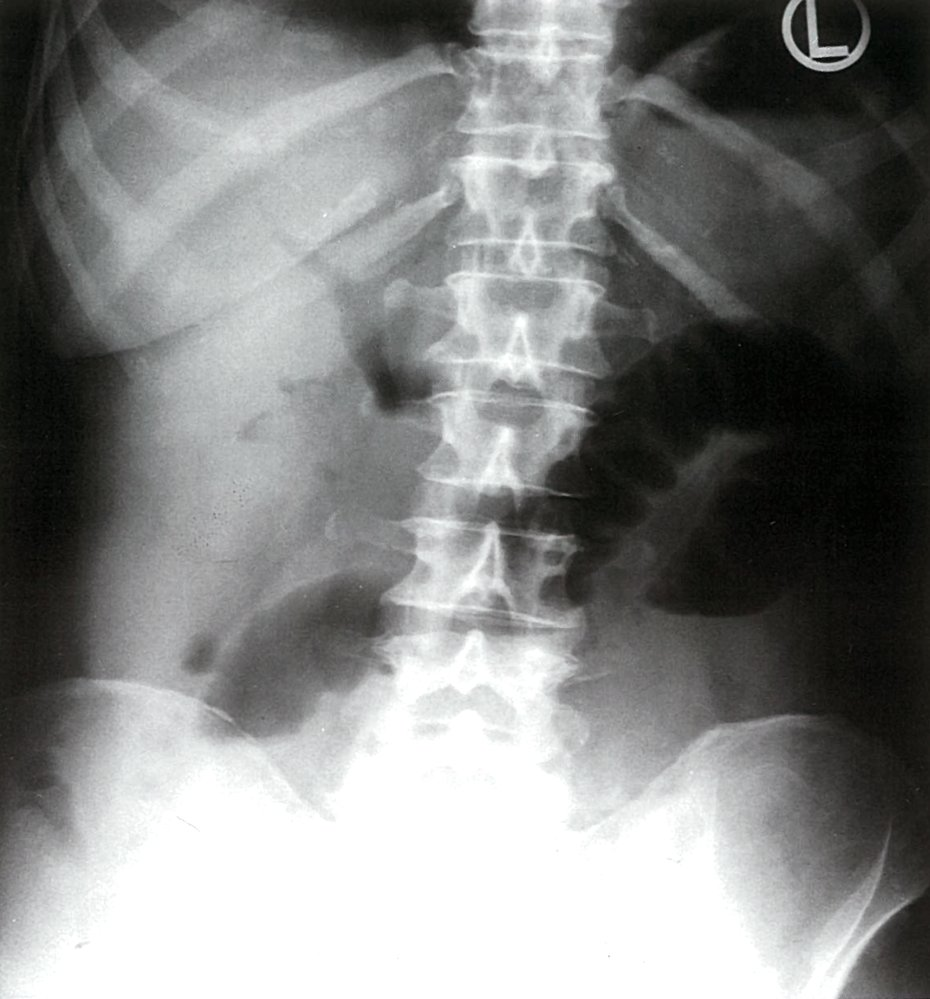
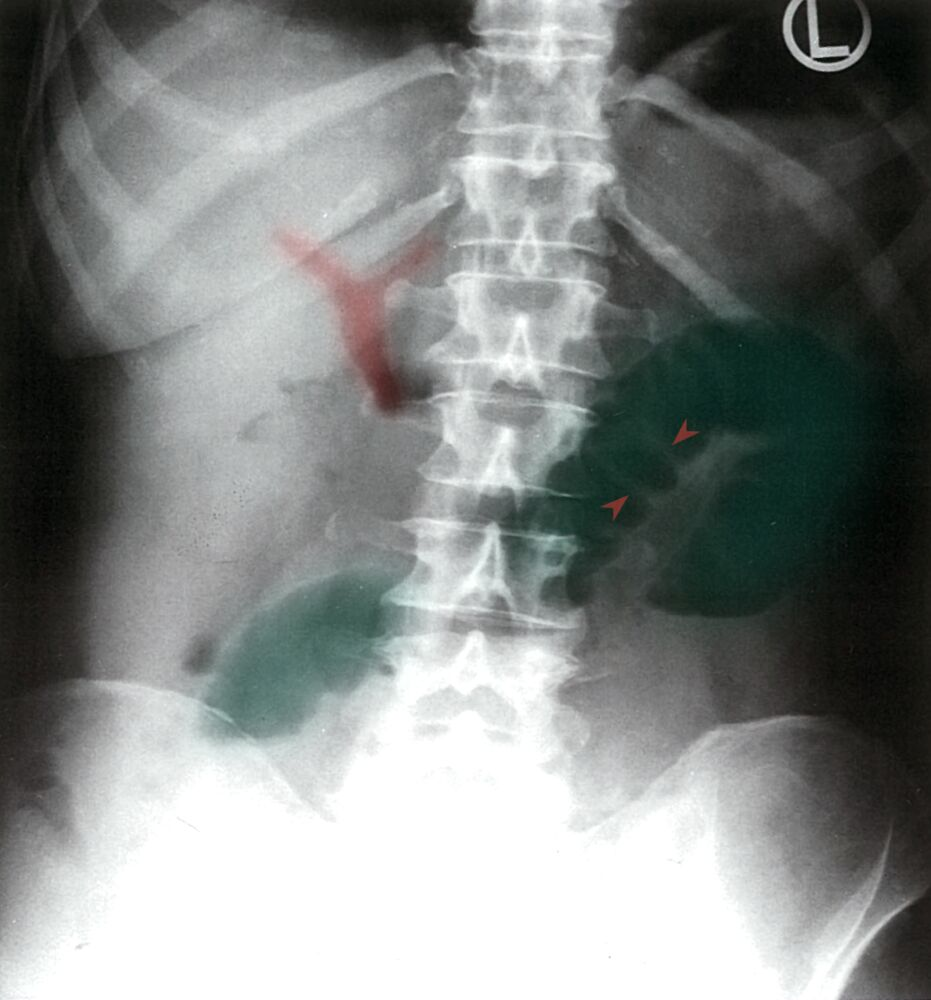
Diagnosis is based on the Rigler triad: imaging findings of small bowel obstruction, Gallstones (most commonly in iliac fossa), and pneumobilia.
Air can move up toward the biliary ducts through a cholecystoenteric fistula.