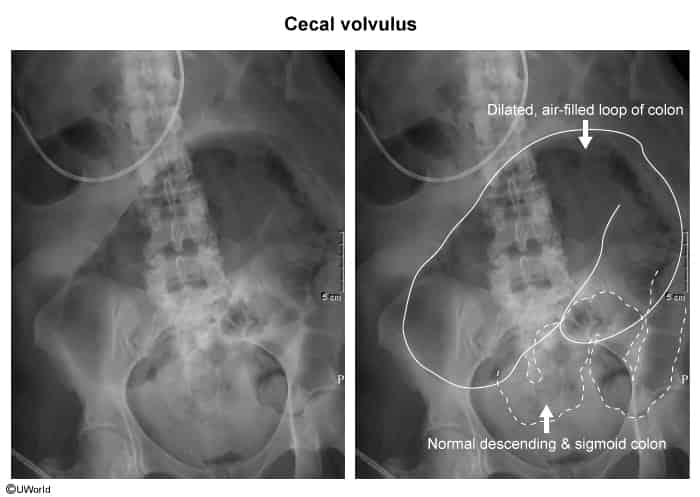
Sigmoid Volvulus: Diff by older age, chronic constipation, and XR showing coffee bean apex pointing to the RUQ (base in LLQ).
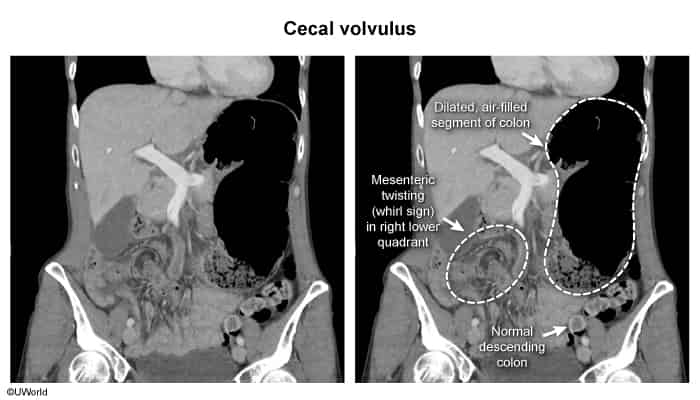
Small Bowel Obstruction (SBO): Diff by absence of cecal twisting/whirl sign on CT, though clinical presentation is virtually identical.
Acute Appendicitis: Diff by localized RLQ pain (McBurney’s point), lack of massive abdominal distention, and CT showing inflamed appendix rather than rotated cecum.
Cecal Cancer: Diff by subacute/chronic presentation, weight loss, iron deficiency anemia, and CT showing a mass rather than a volvulus.
Management
Endoscopic Decompression:
Contraindicated / Avoided: Colonoscopy is rarely effective and carries a high risk of perforation; should not be attempted.
All Patients (Stable or Unstable):
Emergent/Urgent Surgical Intervention is required.
Bowel is Viable: Right hemicolectomy (or ileocecal resection) w/ primary anastomosis. Alternatively, cecopexy (suturing cecum to abdominal wall) if pt is highly unstable, though recurrence risk is higher.
Bowel is Non-viable (Gangrenous/Ischemic/Perforated): Right hemicolectomy w/ end ileostomy (resection w/ primary anastomosis is avoided in unstable pts or severe peritoneal contamination).
Complications
Early bowel ischemia and gangrene (occurs faster than in sigmoid volvulus).
Cecal perforation and peritonitis.
Septic shock.
Recurrence (if cecopexy is performed instead of resection).