CT scan of abdomen/pelvis with water-soluble (oral/rectal/IV) contrast (e.g., Gastrografin). c
High-Yield: Avoid barium contrast due to risk of severe, chemical barium peritonitis if it leaks into the peritoneal cavity.
Key Findings: Free extraluminal air, fluid collections/abscesses surrounding the anastomosis, or direct contrast extravasation.
Esophageal leak variant: Diagnosed via water-soluble contrast esophagram or chest/abdomen CT with oral contrast.
Labs:
Leukocytosis (or leukopenia/bandemia in severe sepsis).
Elevated CRP, procalcitonin, and lactic acid (marker of hypoperfusion).
Confirmatory (Unstable Patient):
Surgical exploration (laparoscopy or laparotomy) acts as both diagnostic and therapeutic gold standard for hemodynamically unstable patients or those with diffuse peritonitis.
Differential Diagnostics
Postoperative Pelvic/Abdominal Abscess:
Differentiation: Presents with fever/leukocytosis but without active, free-flowing luminal contrast extravasation on CT. Often managed with percutaneous drainage alone; does not require taking down the anastomosis.
Superficial/Deep Surgical Site Infection (SSI):
Differentiation: Limited to abdominal wall/subcutaneous tissue; lacks signs of deep peritonitis or intraperitoneal contrast extravasation on CT.
Postoperative Ileus / Small Bowel Obstruction (SBO):
Differentiation: Presents with abdominal distension and vomiting, but lacks signs of systemic sepsis (no high-grade fever, severe leukocytosis) and lacks extraluminal contrast/free air on CT.
Pulmonary Embolism (PE):
Differentiation: Presents with sudden dyspnea and tachycardia, but lacks abdominal signs/peritonitis. Diagnosed via CTPA.
Management
Step 1: Emergency Stabilization (All Patients):
Make patient NPO, initiate aggressive IV fluid resuscitation, place NG tube for decompression, and administer immediate broad-spectrum IV Abx (e.g., Piperacillin/Tazobactam or Carbapenem).
Step 2: Definitive Treatment (Based on Hemodynamic Stability):
Hemodynamically Unstable / Diffuse Peritonitis:
Immediate Surgical Exploration (emerg-lap).
Takedown of the leaky anastomosis, proximal diversion stoma creation (e.g., Hartmann’s procedure for rectosigmoid leaks), extensive abdominal lavage/washout, and drain placement.
High-Yield: Never attempt primary re-anastomosis in a septic, inflamed abdominal field.
Hemodynamically Stable + Contained/Small Leak:
Conservative management: Strict bowel rest (NPO), nutritional support via total parenteral nutrition (TPN), and IV Abx.
CT-guided percutaneous (IR) drainage of any localized peri-anastomotic fluid collections.
History: Pt reports sudden “giving way” or “popping” sensation in the abdominal wall, often precipitated by coughing, straining, or lifting.
Physical Exam:
Profuse, copious “straw-colored” (serosanguineous) fluid discharge from the surgical wound (highly predictive of fascial separation). c
Primarily peritoneal fluid mixed with inflammatory exudate. Post-laparotomy, the peritoneal membrane is irritated and inflamed, leading to hypersecretion of protein-rich serous fluid.
Bulging of the abdominal wall or palpable fascial defect beneath an intact skin layer.
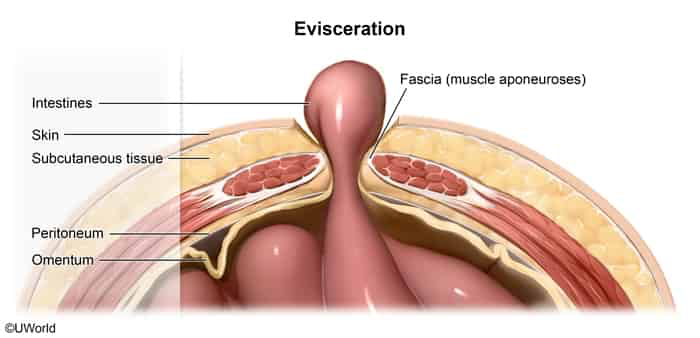
Wound separation without protrusion of underlying abdominal organs (if organs protrude, it has progressed to evisceration).
Management
Immediate Stabilizing Measures:
Apply sterile, saline-soaked (moist) dressings over the wound to prevent desiccation.
Place an abdominal binder (if evisceration is NOT present) to reduce tension on the abdominal wall.
Keep pt NPO, initiate IV hydration, and administer broad-spectrum IV Abx.
Encourage strict bed rest and avoid any maneuvers that increase intra-abdominal pressure.
Surgical Intervention (First-Line/Definitive):
Urgent return to the Operating Room (OR) for wound exploration, debridement of necrotic/infected tissue, and primary fascial re-closure using heavy, non-absorbable retention sutures. c
Refractory/Infected Management:
If gross contamination or severe infection (e.g., necrotizing fasciitis) is present, the wound must be debrided and left open (e.g., negative pressure wound therapy [wound VAC] or temporary abdominal closure devices) for delayed primary closure.
Complications
Evisceration (immediate progression of untreated dehiscence). c
Immediate Bedside Stabilization:
NPO immediately.
Never attempt to push the exposed bowel back into the abdomen at the bedside (risk of bowel perforation or ischemia).
Cover the exposed bowel with sterile, warm, saline-moistened dressings to prevent bowel desiccation, necrosis, and heat loss.
Initiate aggressive IVFs (isotonic crystalloids) to maintain hemodynamic stability.
Administer broad-spectrum IV Abx (e.g., Cefazolin + Metronidazole or Piperacillin-Tazobactam) to prevent peritonitis.
Give adequate IV analgesics and antiemetics (to prevent retching or vomiting, which increases intra-abdominal pressure).
Definitive Treatment:
Emergent surgical exploration and closure in the OR.
Peritonitis or intra-abdominal abscess.
Sepsis and multi-organ dysfunction syndrome (MODS).
Incisional hernia (occurs in up to 30% of closed dehisced wounds).