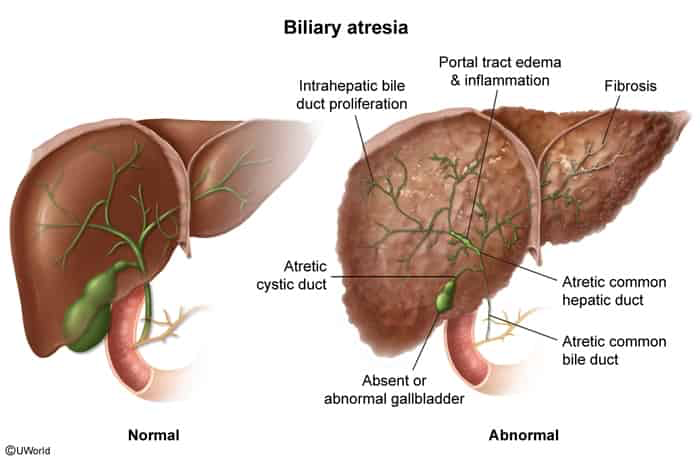
Idiopathic, progressive fibroinflammatory obliteration of the extrahepatic biliary tree.
Onset: Neonates (typically presenting at 2–8 weeks of life).
Epidemiology: Most common indication for pediatric liver transplantation.
Clinical Features
Healthy at birth with normal birth weight.
Progressive jaundice appearing within the first 2–8 weeks.
Acholic (pale/clay-colored) stools due to the absence of conjugated bilirubin in the gut.
Dark (tea-colored) urine due to renal excretion of water-soluble conjugated bilirubin.
Hepatomegaly, firm liver on palpation.
Splenomegaly (late sign indicating portal HTN).
FTT if diagnosis or treatment is delayed.
Diagnosis
Initial Labs: ↑ Direct (conjugated) bilirubin (defined as > 1.0 mg/dL if total < 5.0, or > 20% of total), ↑ GGT, ↑ ALP.
Initial Imaging: RUQ US shows absent or small/hypoplastic gallbladder, “triangular cord sign” (fibrous cone of echogenic tissue at the porta hepatis).
Screening/Next step: HIDA scan (hepatobiliary scintigraphy) showing normal liver uptake of tracer but failure of excretion into the duodenum after 24 hours (often pre-treated with phenobarbital to stimulate bile secretion).
Biopsy: Percutaneous liver biopsy shows bile duct proliferation, portal tract fibrosis, and bile plugs.
Breast Milk Jaundice: Differentiated by unconjugated (indirect) hyperbilirubinemia, normal-colored stools, and onset after the first week of life.
Neonatal Hepatitis: Differentiated by a patent biliary tree on HIDA scan and a liver biopsy showing giant cell transformation rather than ductal proliferation.
Choledochal Cyst: Differentiated by RUQ US showing cystic dilation of the biliary tree.
Galactosemia: Differentiated by systemic symptoms (vomiting, cataracts, hypoglycemia, hypotonia) and (+) urine reducing substances.
Alagille Syndrome: Differentiated by syndromic features (butterfly vertebrae, peripheral pulmonic stenosis, triangular facies) and bile duct paucity on liver biopsy.
Management
First-line (Surgical): Kasai procedure (hepatoportoenterostomy) to restore biliary drainage.
Must be performed early (ideally < 8 weeks of age) to prevent progressive liver damage.