Epidemiology
Etiology
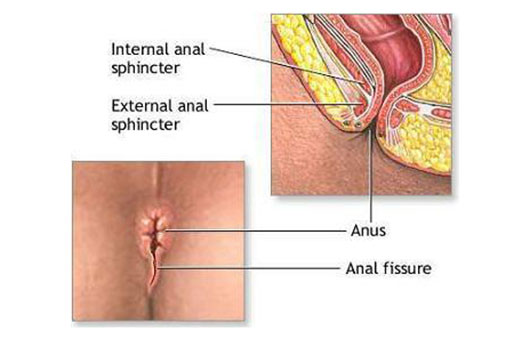
- Location: 90% of all anal fissures located at the posterior commissure (6 o’clock in the lithotomy position)
- Due to the relatively poor perfusion of the posterior anal canal, which makes its mucosa sensitive to trauma and slows healing times
- Due to the relatively poor perfusion of the posterior anal canal, which makes its mucosa sensitive to trauma and slows healing times
Pathophysiology
Clinical features
<% tp.file.cursor() %>
Diagnostics
<% tp.file.cursor() %>
Differential diagnostics
Proctalgia fugax
- Pathophysiology & Triggers: Transient spasm of rectal smooth muscle; strongly associated with stress, anxiety, and IBS.
- Clinical Presentation: Sudden, severe, sharp/cramping rectal pain lasting seconds to minutes (< 30 min), often occurring at night; pt is asymptomatic between episodes. c
- Physical Exam: DRE is normal with no local tenderness, masses, or fissures.
- Diagnosis: Clinical diagnosis of exclusion; ruling out organic pathology with a normal physical exam is key.
- Key Differentials:
- Levator ani syndrome: Dull, chronic pain lasting > 30 min (worse with sitting) + tenderness on palpation of levator ani during DRE.
- Anal fissure: Severe pain during/after defecation + hematochezia + visible tear.
- Thrombosed hemorrhoid: Constant, acute pain + visible purple perianal nodule.
- Management:
- 1st-line: Reassurance of benign nature; warm sitz baths.
- 2nd-line (acute): Inhaled salbutamol (albuterol) (relaxes smooth muscle); topical nitroglycerin.
Treatment
- First-line (Conservative/Supportive):
- High-fiber diet and fiber supplements (e.g., psyllium).
- Stool softeners (e.g., docusate) and aggressive oral hydration.
- Sitz baths (warm water relaxes the internal anal sphincter and improves local microvascular perfusion).
- Second-line (Topical Vasodilators):
- Topical nitroglycerin (NTG) or calcium channel blockers (CCB, e.g., 2% diltiazem cream) applied locally to the anus to relieve sphincter spasm and facilitate healing (Note: NTG can cause systemic headaches). c
- Topical anesthetics (e.g., lidocaine) for temporary symptomatic relief.
- Botulinum toxin injection into the internal anal sphincter (if topicals fail).
- Third-line / Refractory (Surgical):
- Lateral internal sphincterotomy (LIS): Surgical division of the internal anal sphincter. Reserved for chronic, medically refractory cases. Highly effective but carries a minor long-term risk of fecal/flatus incontinence.
- Note: Avoid surgical sphincterotomy in pts with Crohn’s disease due to a high risk of poor wound healing and fecal incontinence.