Epidemiology
Etiology
Pathophysiology
Heavy ethanol consumption → intrahepatic oxidative damage → recruitment of neutrophils to the liver
Clinical features
- Rapid onset of jaundice, anorexia, fever, and tender hepatomegaly.
- RUQ pain and abdominal distension (due to ascites).
- Physical Exam:
- Scleral icterus and jaundice.
- Stigmata of chronic liver disease (spider angiomata, palmar erythema, gynecomastia, caput medusae).
- Proximal muscle wasting (temporalis, deltoid).
- Asterixis/altered mental status (suggests hepatic encephalopathy).
Diagnostics
Initial/Key Labs
- AST:ALT ratio ≥ 2:1 (AST and ALT are typically <500 U/L; AST rarely exceeds 300 U/L).
- Macrocytic anemia (MCV > 100 fL, exacerbated by direct EtOH toxicity and folate deficiency).
- Neutrophilic leukocytosis (can mimic bacterial infection).
- Elevated direct bilirubin (>3 mg/dL) and GGT
- Prolonged PT/INR and hypoalbuminemia (impaired synthetic function).
Mnemonic
AST > ALT in alcoholic hepatitis: Remember “make a toAST with alcohol!”
Liver biopsy
- Marked intrahepatic neutrophilic infiltration
- Hepatocellular ballooning
- Mallory bodies
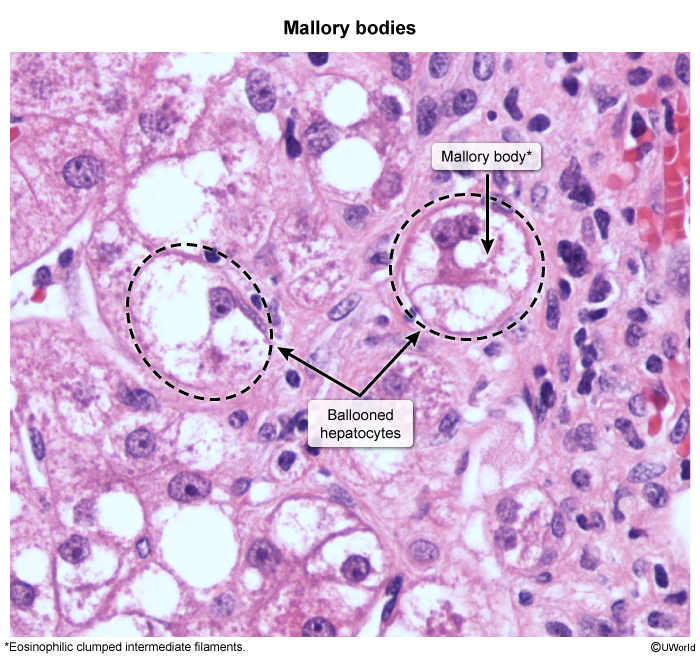
- Steatosis