Description: an acute life-threatening necroinflammatory disorder of the gallbladder, usually seen in critically ill patients, that is not associated with Gallstones
Etiology: conditions predisposing to bile stasis and reduced perfusion of the gallbladder
Clinical features: similar to acute calculous cholecystitis
Clinical features
Diagnostics
Initial Test: RUQ Ultrasound (US).
Key findings: GB wall thickening (>4 mm), pericholecystic fluid, sonographic Murphy sign, and presence of gallstones/sludge.
Key Labs: Leukocytosis (with left shift). LFTs (AST, ALT, Bilirubin, Alk Phos) and amylase/lipase are typically normal (unless complicated by choledocholithiasis or pancreatitis).
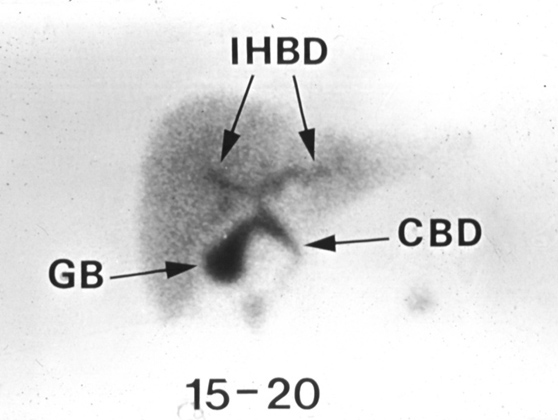
Gold Standard / Confirmatory Test (if US equivocal): HIDA scan (Cholescintigraphy).
Definition: Nuclear medicine imaging modality utilizing a radiotracer (typically technetium-99m labeled iminodiacetic acid analogs) to assess the functional patency of the hepatobiliary system.
Positive result: Non-visualization of the GB after 1–4 hours due to cystic duct obstruction.
Treatment
First-line (Stabilization):
NPO, IVF, analgesics (NSAIDs or opioids).
IV Abx: Cover Gram-negatives and anaerobes (e.g., Ceftriaxone + Metronidazole, or Pip/Tazo).
Definitive Management:
Early laparoscopic cholecystectomy (typically within 72 hours of admission). c
Refractory/High-Risk Patients:
Percutaneous cholecystostomy (drainage tube placement for pts unfit for general anesthesia).
Complications
Chronic cholecystitis
Clinical features: recurrent symptoms similar to acute cholecystitis but typically less severe and often self-limiting
Complications
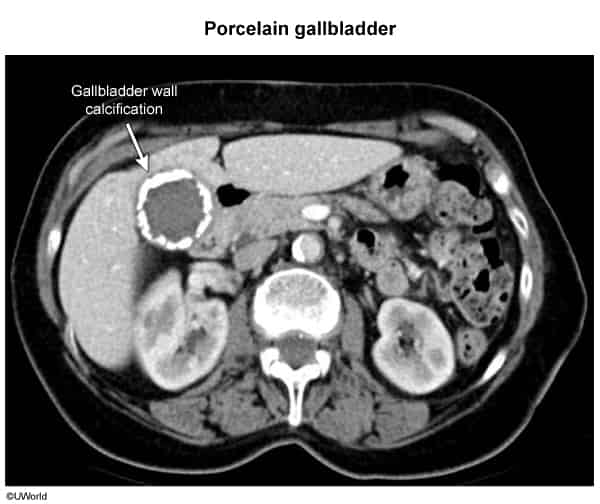
Porcelain gallbladder
Definition: calcification of the gallbladder wall due to chronic inflammation
Imaging (x-ray or noncontrast CT abdomen): focal or diffuse hyperdensity (radiopaque appearance) of the gallbladder wall
Clinical significance: a risk factor for gallbladder cancer
Treatment: conservative management or laparoscopic cholecystectomy based on symptoms, pattern of gallbladder calcification, and comorbidities
Emphysematous cholecystitis
Infection by gas-forming orgs (e.g., Clostridium perfringens), common in diabetic patients.
Findings: Gas in gallbladder wall/lumen on imaging.
Management: Urgent cholecystectomy + Abx (must cover anaerobes). c