Epidemiology
Etiology
Pathophysiology
DKA
- Primarily a complication of Type 1 Diabetes Mellitus, but can occur in T2DM.
- Caused by a profound insulin deficiency, often precipitated by the “5 I’s”: Infection (most common), Ischemia (MI, CVA), Infarction, Inadequate insulin, and Initial presentation of diabetes.
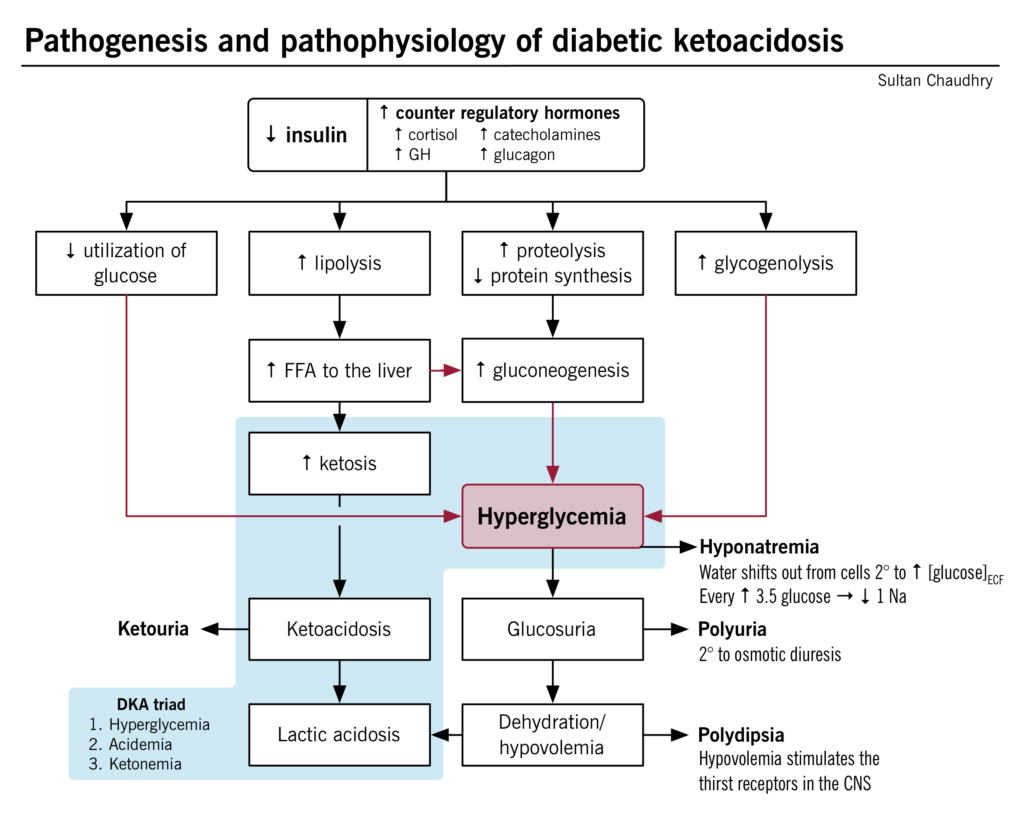
- ↓ Insulin → unopposed counter-regulatory hormones (glucagon, cortisol, catecholamines).
- This hormonal imbalance leads to:
- ↑ Hepatic gluconeogenesis & glycogenolysis → Hyperglycemia.
- ↑ Unrestrained lipolysis → breakdown of triglycerides into free fatty acids.
- The liver converts fatty acids into ketone bodies (β-hydroxybutyrate and acetoacetate), leading to ketosis and metabolic acidosis.
- Hyperglycemia causes osmotic diuresis, leading to severe dehydration and electrolyte loss.
- Insulin deficiency → hyperosmolality → K+ shift out of cells + lack of insulin to promote K+ uptake → intracellular K+ depleted → total body K+ deficit despite normal or even elevated serum K+
Tip
There is a total body potassium deficit in DKA. This becomes important during treatment, when insulin replacement leads to rapid potassium uptake by depleted cells and patients may require potassium replacement.
HHS
- Primarily affects patients with type 2 diabetes
- The pathophysiology of HHS is similar to that of DKA.
- However, in HHS, there are still small amounts of insulin being secreted by the pancreas, and this is sufficient to prevent DKA by suppressing lipolysis and, in turn, ketogenesis.
- HHS is characterized by symptoms of marked dehydration (and loss of electrolytes) due to the predominating hyperglycemia and osmotic diuresis.
Clinical features
Diagnostics
Tip
- DKA is the diagnosis in patients with type 1 diabetes who have hyperglycemia, ketonuria, and high anion gap metabolic acidosis with decreased bicarbonate!
- HHS is the diagnosis in patients with type 2 diabetes who have hyperglycemia and hyperosmolality!
- Bedside/Initial Evaluation:
- Capillary blood glucose (BG) and venous blood gas (VBG) (VBG is preferred; ABG is no longer routinely required to assess acid-base status).
- Capillary/plasma beta-hydroxybutyrate (BHB): Superior to urine ketones (urine acetoacetate can remain false-positive during recovery).
- Diagnostic Comparison:
| Parameter | Diabetic Ketoacidosis (DKA) | Hyperosmolar Hyperglycemic State (HHS) |
|---|---|---|
| Blood Glucose | (or prior history of DM irrespective of BG to account for euglycemic DKA) | |
| Venous pH | (Mild: 7.25–7.30; Mod: 7.00–7.24; Severe: ) | |
| Serum Bicarbonate | ||
| Ketones | Elevated plasma BHB () or urine ketones | Absent or minimal |
| Effective Osmolality | Variable | |
| Anion Gap | Elevated () | Variable (typically normal) |
| Mental Status | Alert to stupor/coma (in severe DKA) | Stupor or coma |
- Corrected Sodium: Hyperglycemia draws water intracellularly, causing pseudohyponatremia.
- Correction Formula: Corrected (use 2.4 if BG ).
- If corrected is low, it indicates a severe free water deficit.
- Despite total body depletion, initial serum is often normal or elevated because:
- Acidemia: ions enter cells, shifting out into the extracellular fluid (ECF).
- Insulin Deficiency: Without insulin, the ATPase pump is underactive, preventing from entering cells.
- Hyperosmolality: Water moves out of cells, dragging with it (solvent drag).
Treatment
Must be managed systematically with parallel focus on fluids, potassium, and insulin.
1. Fluid Resuscitation (First Step)
- Goal: Restore intravascular volume and renal perfusion. Start fluids before insulin.
- Initial Fluid: 0.9% NaCl (normal saline) or balanced crystalloids (e.g., Lactated Ringer’s) at 500–1000 mL/hr for the first 2–4 hours.
- Note: Use smaller fluid boluses (e.g., 250 mL) in patients with CHF or ESRD to avoid fluid overload.
- Subsequent Fluid: Based on corrected sodium and hydration status:
- If corrected is high/normal: Switch to 0.45% NaCl (half-normal saline) at 250–500 mL/hr.
- If corrected is low: Continue 0.9% NaCl at 250–500 mL/hr.
- Adding Dextrose:
- In DKA: Add 5% to 10% Dextrose (in 0.45% NaCl) once BG falls . This allows continued insulin infusion to clear ketones without causing hypoglycemia.
- In HHS: Add 5% to 10% Dextrose once BG falls .
2. Potassium Management (Crucial Safety Step)
Insulin shifts intracellularly, causing a rapid drop in serum levels. Always check before starting insulin.
- : HOLD insulin. Administer IV potassium chloride (10–20 mEq/hr) until before initiating insulin.
- 3.5–5.3 mEq/L: Give insulin. Add 20–30 mEq to each liter of IV fluids to maintain serum between 4.0 and 5.0 mEq/L.
- : Give insulin. Do not add potassium to IV fluids. Monitor every 2–4 hours.
3. Insulin Therapy
- Route: Continuous IV insulin infusion is preferred for moderate/severe DKA and HHS.
- Mild/moderate DKA: Can be managed in non-ICU settings with SC rapid-acting insulin analogs (every 1–2 hours).
- Dosing:
- DKA: Start IV regular insulin at 0.1 units/kg/hr.
- HHS: Start IV regular insulin at 0.05 units/kg/hr (slower rate to avoid rapid shifts in osmolality, unless mixed features with DKA are present, which requires 0.1 units/kg/hr).
- Target rate of glucose decline: Aim for 50–70 mg/dL/hr (maximum 90–120 mg/dL/hr in HHS to prevent cerebral edema).
4. Bicarbonate Therapy
- Routine Use: Not recommended (can worsen intracellular acidosis, cause hypokalemia, and delay ketosis resolution).
- Indication: Only consider if severe acidemia (pH < 6.9–7.0) with hemodynamic instability or life-threatening hyperkalemia.
DKA Resolution
- Criteria: BG AND at least one of:
- Venous pH
- Serum bicarbonate
- Plasma BHB (ketones)
- Note: Anion gap is no longer the primary marker of resolution due to hyperchloremic acidosis from large volume saline.
- Transition to Subcutaneous Insulin:
- Never stop IV insulin abruptly.
- Administer basal SC insulin 2–4 hours before discontinuing the IV insulin infusion to prevent rebound ketosis.
- If already taking basal insulin home regimen, it can be continued at the usual dose during IV insulin treatment.
HHS Resolution
- Criteria: Effective osmolality AND patient returns to baseline mental status.