Postoperative complications
Cardiovascular & Pulmonary Complications
- Postoperative MI
- Usually POD 2-3. Often silent (no chest pain) due to analgesia/anesthesia. c
- Risk Factors: Pre-existing CAD, CHF, CKD, diabetes mellitus, advanced age (> 65), and high-risk surgical procedures (e.g., vascular, prolonged open abdominal/thoracic surgeries).
- Pathophysiology: Usually due to surgical stress (↑ catecholamines causing ↑ myocardial oxygen demand/tachycardia) superimposed on baseline CAD (demand ischemia/Type 2 MI), or plaque rupture (Type 1 MI) secondary to hypercoagulability/inflammation.
- Presentation: Hypotension, arrhythmias, dyspnea, new-onset HF.
- Dx: ECG, Troponins.
- Tx: PCI or medical management (Aspirin, statin, beta-blocker if hemodynamically stable).
- ARDS (Acute Respiratory Distress Syndrome)
- Post-trauma, massive transfusion, or sepsis.
- Dx: Bilateral opacities on CXR, PaO2/FiO2 < 300.
- Tx: Mechanical ventilation with low tidal volumes (6 mL/kg) & PEEP.
- Postoperative atelectasis
-
Most common after thoracic or upper abdominal surgeries.
-
PE: ↓ breath sounds, dullness to percussion, basilar crackles.
-
Management
- First-line / Prevention: Incentive spirometry (NBS & best preventive measure), early ambulation. c
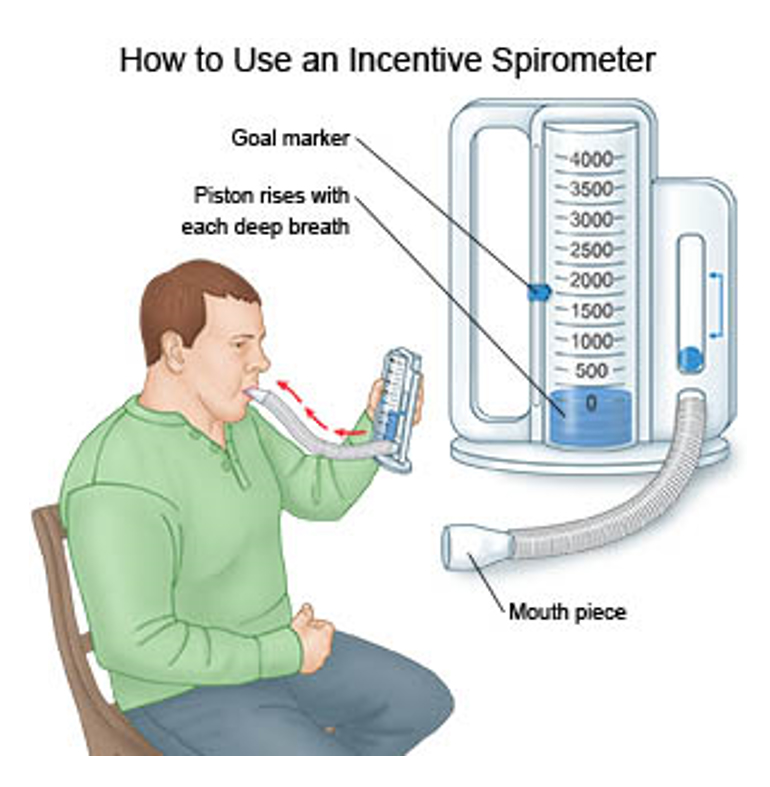
- Second-line: Optimize pain control (e.g., epidural/PCA to allow deep breaths).
- Refractory: CPAP/BiPAP for persistent hypoxemia.
- First-line / Prevention: Incentive spirometry (NBS & best preventive measure), early ambulation. c
-
- Postoperative pneumonia
- Management
- Prevention (Most Important):
- Incentive spirometry, deep breathing exercises. c
- Early mobilization.
- Adequate post-op pain control (epidural/regional blocks preferred over high-dose opioids to prevent hypoventilation).
- First-line (Empiric Antibiotics): Must target Gram-negatives (including Pseudomonas) and Gram-positives (including MRSA) based on local antibiogram.
- Pseudomonas coverage (choose 1): Piperacillin-tazobactam (Zosyn), Cefepime, or Meropenem.
- MRSA coverage (choose 1): Vancomycin or Linezolid.
- Second-line / De-escalation: Narrow Abx spectrum based on sputum/blood culture results after 48-72 hours. Duration: Typically 7 days for uncomplicated HAP.
- Supportive: Supplemental (maintain ), chest physiotherapy, aggressive pulmonary toilet.
- Prevention (Most Important):
- Management
Acute Postoperative Mediastinitis
- Epidemiology & Risk Factors
- < 14 days post-median sternotomy (CABG/valves).
- Orgs: S. aureus, S. epidermidis.
- Risks: DM, obesity, smoking, reoperation.
- Clinical Features
- Fever, tachycardia, purulent wound drainage.
- Buzzword: Sternal instability (“clicking” or “rocking” w/ breathing).
- Diagnosis
- Initial: Blood & wound cx, CBC (↑ WBC).
- Imaging: CT Chest w/ contrast (mediastinal fluid/gas). Note: Small amt of pneumomediastinum on CXR is normal < 14 days post-op; worsening gas is pathologic.
- Confirmatory: Surgical exploration w/ positive cx.
- Differential Diagnostics
- Superficial Skin Infection: Intact sternum (no clicking), no systemic toxicity.
- Postpericardiotomy Syndrome: Autoimmune, weeks-months later. Pleuritic pain, friction rub. Tx: NSAIDs.
- Non-infectious Dehiscence: Sternal clicking without fever or purulence (mechanical failure).
- Management
- Surgical (Immediate): Urgent exploration, debridement, & sternal fixation (muscle flaps). c
- Medical: Empiric IV Abx (Vanco + Cefepime) targeting MRSA/Gram-negatives.
- Ongoing: 4-6 wks IV Abx tailored to cx.
- Complications
- Sepsis / Septic shock (high mortality).
- Sternal osteomyelitis.