Cholesterol embolization syndrome is a condition in which cholesterol crystals dislodge from atherosclerotic plaques and enter the bloodstream, blocking small to medium arteries in various organs.
Epidemiology
Etiology
- Pts w/ severe, diffuse atherosclerosis (HTN, hyperlipidemia, smoking).
- Typically occurs days to weeks following a vascular procedure (e.g., PCI, angiography, aortic surgery). c
- Delayed inflammatory occlusion of microvessels caused by small cholesterol crystals, not just mechanical occlusion
- Can be triggered by initiation of anticoagulation or thrombolytics (destabilizes plaques).
- Rarely spontaneous.
Pathophysiology
Atherosclerotic cardiovascular disease → rupture of atherosclerotic plaque (most commonly from the aorta) → blockage and inflammation of small to medium arteries by cholesterol crystals → formation of multiple small peripheral, muscular, or visceral emboli → end-organ damage
Clinical features
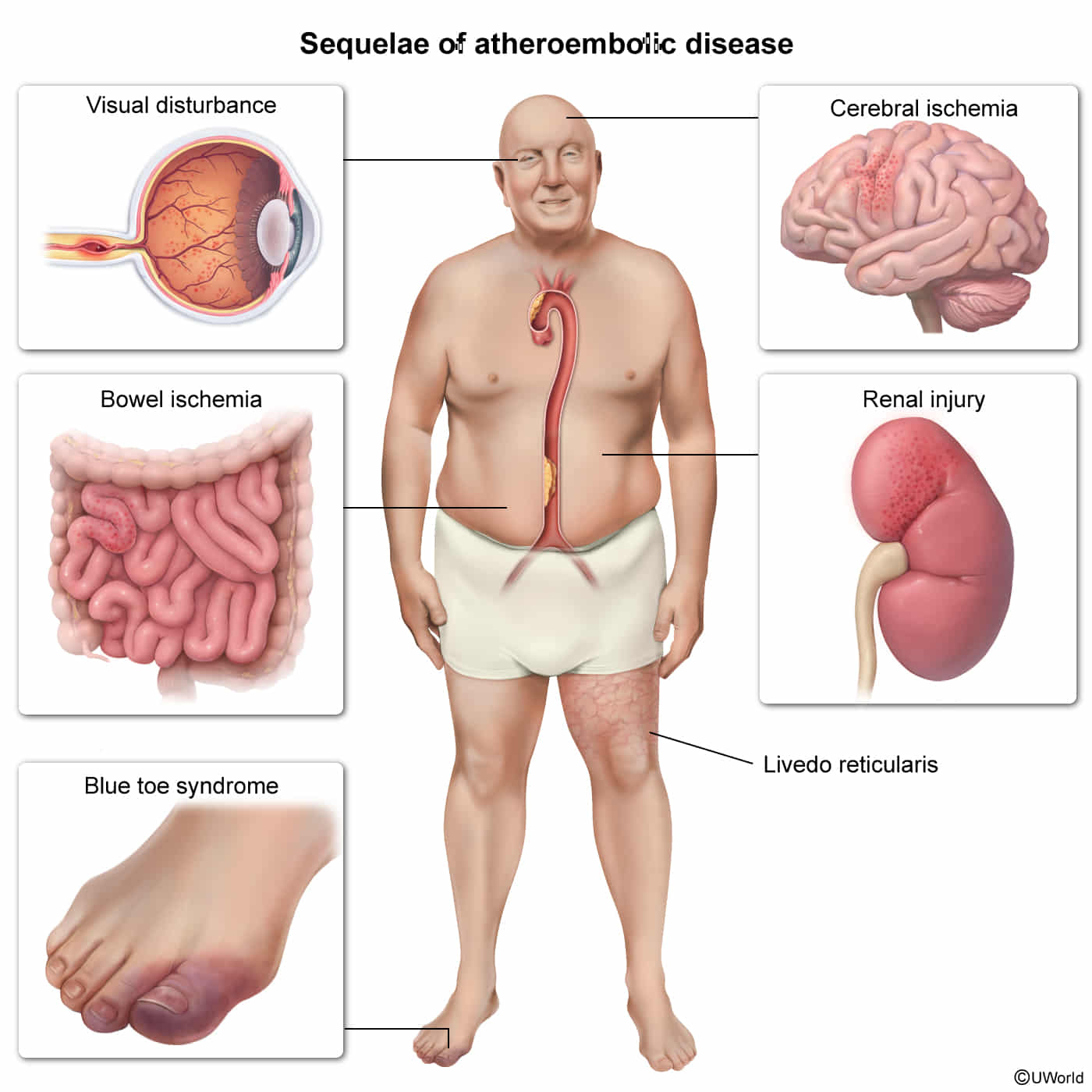
- Cutaneous: Livedo reticularis, “blue toe syndrome” (cyanotic toes w/ intact peripheral pulses), gangrene, skin ulcers. c2

- Renal: Acute or subacute kidney injury (AKI) typically presenting 1-2 weeks post-procedure.
- Ocular: Hollenhorst plaques (bright yellow, refractile cholesterol plaques in retinal arterioles).
- GI: Intestinal ischemia (abd pain, bleeding).
- Neuro: TIA, stroke, amaurosis fugax.
- Systemic: Fever, myalgias, weight loss (mimics systemic vasculitis).
Diagnostics
- Initial: Clinical diagnosis based on classic triad (recent vascular intervention, subacute AKI, livedo reticularis/“blue toes”).
- Key Labs:
- Eosinophilia & eosinophiluria (due to IL-5 activation by exposed atheroma elements). c
- Hypocomplementemia (low C3, C4 due to alternative pathway activation by atheroemboli).
- Elevated serum Cr and ESR.
- Urinalysis: Typically benign or mild proteinuria/hematuria (no RBC casts).
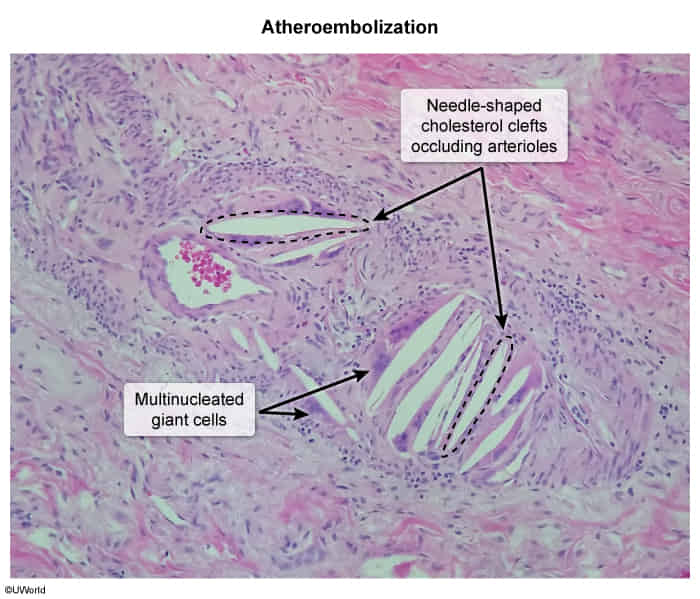
- Confirmatory/Gold Standard: Skin or renal biopsy demonstrating needle-shaped cholesterol clefts (biconvex “ghosts” of cholesterol crystals washed out during tissue fixation) occluding small arteries, accompanied by intravascular thrombus and foreign-body giant cell reaction.
Treatment
- Supportive & Preventive (First-line):
- Discontinue offending anticoagulants/thrombolytics immediately to prevent further plaque destabilization.
- High-intensity statin therapy (stabilizes plaques, reduces local inflammation, promotes regression).
- BP control (typically utilizing ACEi or ARBs for renal protection).
- Avoid future invasive vascular/arterial procedures.
- Supportive renal therapy (avoiding nephrotoxins, careful fluid balance, dialysis if ESRD develops).
- Refractory/Severe (Cutaneous/Systemic):
- Corticosteroid therapy (controversial; may reduce local vascular inflammation, but does not improve long-term renal survival).