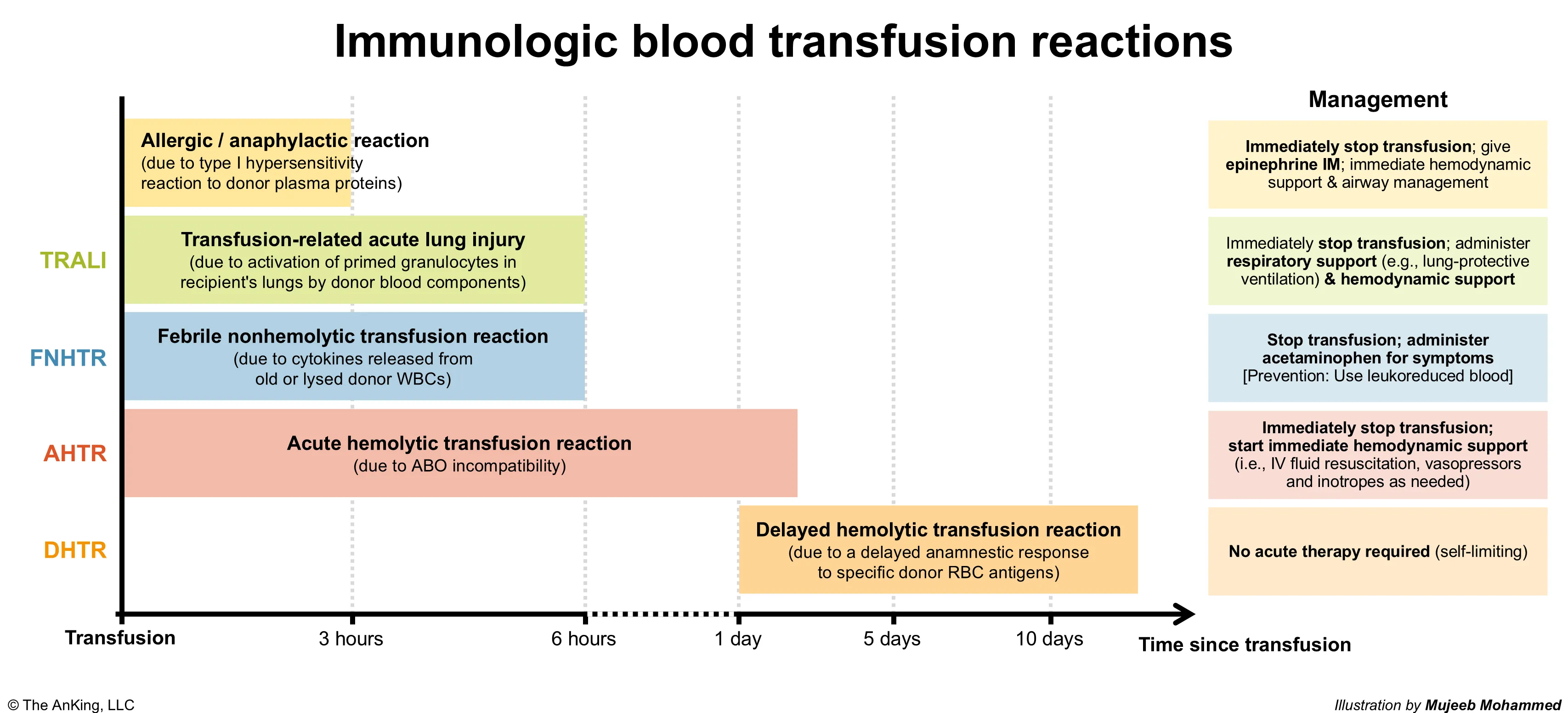
Acute transfusion reaction
Anaphylactic transfusion reaction
- Pathophysiology
- Type I hypersensitivity reaction in which preformed IgE antibodies on the surface of mast cells bind to donor plasma proteins (commonly donor IgA in recipients with IgA deficiency), leading to mast cell degranulation
- Individuals with IgA deficiency should receive IgA-depleted blood products.
- Clinical features: Sudden onset during or up to 3 hours after the transfusion
- Shock, hypotension, wheezing, respiratory distress
- Skin reactions (e.g., pruritus, urticaria)
Pulmonary transfusion complications
Transfusion-Related Acute Lung Injury (TRALI) and Transfusion-Associated Circulatory Overload (TACO) are both characterized by respiratory distress, i.e., dyspnea and hypoxemia, that develops acutely either during or within hours of transfusion.
-
Pathophysiology & Risk Factors
- TRALI: Non-cardiogenic pulmonary edema (ARDS-like). Donor anti-leukocyte antibodies (anti-HLA) attack recipient neutrophils neutrophil trapping in pulmonary capillaries endothelial damage & capillary leak.
- Risk Factors: Plasma-rich products (FFP, platelets); multiparous female donors (↑ anti-HLA Abs from pregnancies).
- TACO: Cardiogenic pulmonary edema. Volume overload from excess volume or rapid infusion rate.
- Risk Factors: Extremes of age (elderly/pediatrics), underlying CV disease (HF), CKD, rapid infusion, large volume.
- TRALI: Non-cardiogenic pulmonary edema (ARDS-like). Donor anti-leukocyte antibodies (anti-HLA) attack recipient neutrophils neutrophil trapping in pulmonary capillaries endothelial damage & capillary leak.
-
Clinical Features (Both occur within 6 hours of transfusion)
- TRALI:
- Hypoxemia & respiratory distress.
- Fever / chills.
- Hypotension.
- Normal/Low JVP, no S3 gallop.
- TACO:
- Hypoxemia & respiratory distress.
- Afebrile (usually).
- Hypertension & tachycardia.
- Elevated JVP, (+) S3 gallop, peripheral edema.
- TRALI:
-
Diagnosis
- Initial: CXR for both.
- TRALI: Bilateral pulmonary infiltrates. Normal cardiac silhouette, no pleural effusions.
- TACO: Bilateral pulmonary infiltrates. Cardiomegaly, pulmonary vascular congestion, Kerley B lines, pleural effusions.
- Key Labs / Imaging:
- BNP/NT-proBNP: Normal in TRALI; Elevated in TACO (or >1.5x pre-transfusion baseline).
- Echocardiography: Normal EF/function in TRALI; Reduced LVEF or elevated filling pressures in TACO.
- Pulmonary Capillary Wedge Pressure (PCWP): Normal ( 18 mmHg) in TRALI; Elevated (> 18 mmHg) in TACO.
- Initial: CXR for both.
-
Differential Diagnostics (Other early transfusion reactions)
- Anaphylactic Reaction: IgA deficiency. Occurs in seconds/minutes. Presents w/ shock, angioedema, wheezing. Diff by absence of bilateral infiltrates on CXR.
- Acute Hemolytic Reaction: ABO incompatibility. Presents w/ fever, flank pain, hemoglobinuria, DIC. Diff by normal CXR, (+) DAT/Coombs, ↑ LDH, ↓ haptoglobin.
- Transfusion-Transmitted Bacterial Infection: Platelets most common. Septic shock, high fever. Diff by normal CXR, (+) blood cultures.
-
Management
- TRALI:
- Stop transfusion immediately (first step for any suspected reaction).
- Respiratory support: Supplemental , intubation/mechanical ventilation (lung-protective strategy) if severe.
- Hemodynamic support: IVF cautiously, vasopressors for hypotension.
- Strictly AVOID diuretics (worsens hypotension/shock).
- TACO:
- Stop transfusion immediately.
- Sit patient upright.
- Respiratory support: Supplemental , CPAP/BiPAP if needed.
- Medical Tx: Loop diuretics (IV Furosemide) nitrates to reduce preload.
- TRALI:
-
Complications
- TRALI: Leading cause of transfusion-related mortality. Long-term pulmonary fibrosis (rare).
- TACO: Respiratory failure, acute decompensated heart failure, death. Often resolves quickly w/ diuresis.
Delayed hemolytic transfusion reaction
Pathophysiology
- Occurs in patients who were previously sensitized to specific RBC antigens during transfusions, pregnancy, or transplantations
- Particularly common in patients receiving repeated transfusions, such as patients with sickle cell disease or thalassemia.
- Usually caused by alloantibodies that form following exposure to minor blood group antigens (e.g., Kidd or D (Rh) antigens)
- Reexposure to the RBC antigens → anamnestic response resulting in an increase in anti-RBC alloantibody titers 24 hours to 28 days following transfusion → binding of alloantibodies to donor RBCs causing extravascular hemolysis
Clinical features
- Onset days or weeks after transfusion (due to the delay in the anamnestic response)
- Most commonly asymptomatic
- May cause:
- Mild fever
- Jaundice
- Anemia
Massive transfusion-related complications
Hypocalcemia
- Resulting from the binding of ionized calcium by citrate (an anticoagulant added to RBC, platelet, FFP, and whole blood transfusion units)
- Normally, following transfusion, citrate is rapidly metabolized to bicarbonate in the liver; however, when large volumes of blood are transfused rapidly, the excess citrate can chelate calcium in the plasma, leading to hypocalcemia due to decreased serum ionized calcium concentration.
- This is most common with very high transfusion rates (eg, >9 units/hr), but it can also be seen at lower rates in patients with underlying hepatic insufficiency (eg, alcohol-associated liver disease).
Hyperkalemia
- Resulting from the lysis of RBCs in stored blood units