Gluteal Region
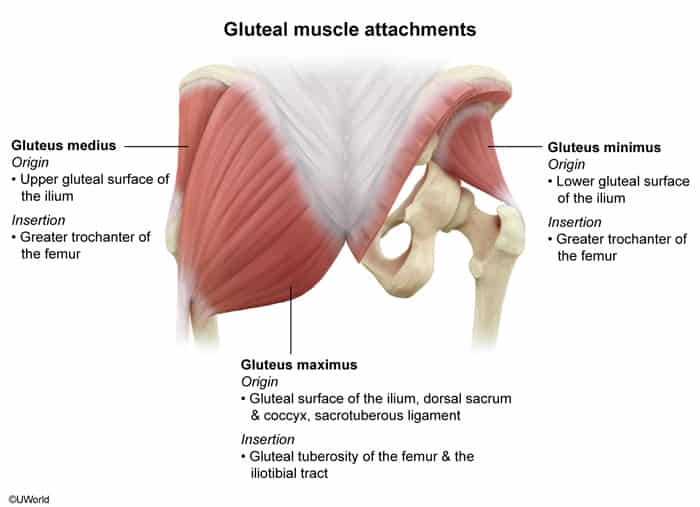
- Gluteus Maximus
- Action: Primary hip extensor (e.g., standing up from chair, climbing stairs).
- Innervation: Inferior Gluteal N. (L5-S2).
- Note: Injury leads to difficulty rising from seated position.
- Gluteus Medius & Minimus
- Action: Hip abduction; stabilizes pelvis during stance phase of gait.
- Innervation: Superior Gluteal N. (L4-S1).
- Clinical: Injury causes Trendelenburg Sign (pelvis drops to the contralateral side when standing on the affected leg).
- Tensor Fasciae Latae (TFL)
- Action: Abduction/Flexion.
- Innervation: Superior Gluteal N.
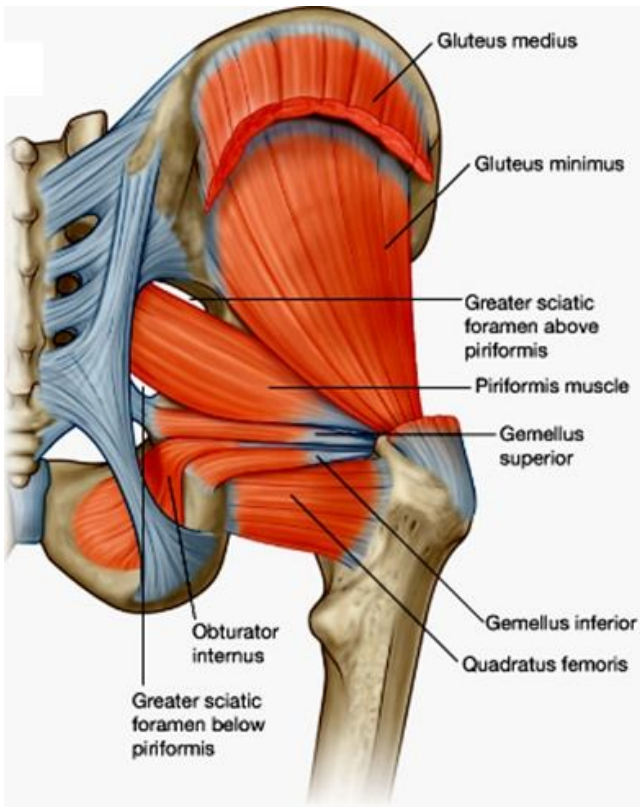
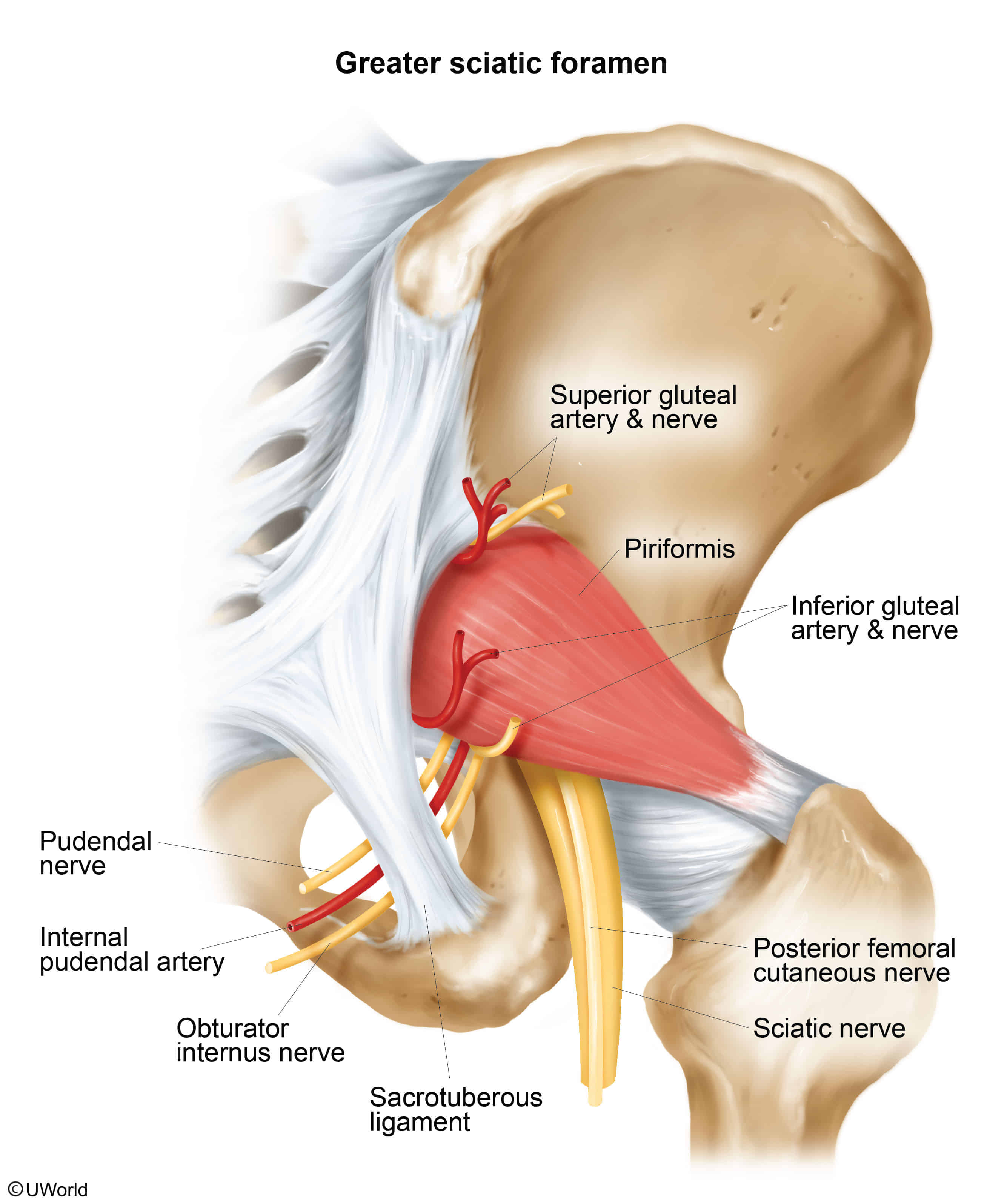
- Piriformis
- Action: External rotation.
- Clinical: Piriformis Syndrome (hypertrophy/inflammation can compress the Sciatic N.).
Thigh: Anterior Compartment (Extensors)
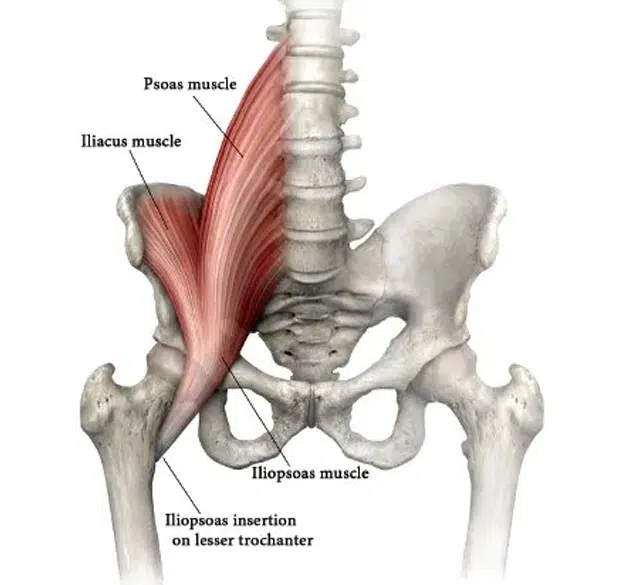
- Iliopsoas (Iliacus + Psoas Major)
- Action: Primary hip flexor.
- Innervation: Lumbar plexus (L1-L3) / Femoral N.
- Clinical: Psoas Abscess (can result from vertebral TB/Pott disease; presents with fever + back pain + limitation of hip extension).
- Quadriceps Femoris (Rectus Femoris, Vastus Lat/Med/Intermed)
- Action: Knee extension; Rectus femoris also flexes hip.
- Innervation: Femoral N. (L2-L4).
- Clinical: Patellar Reflex (L3-L4). Injury leads to inability to extend knee against resistance.
- Sartorius
- Action: Flexes, abducts, laterally rotates hip (FABER position - cross-legged).
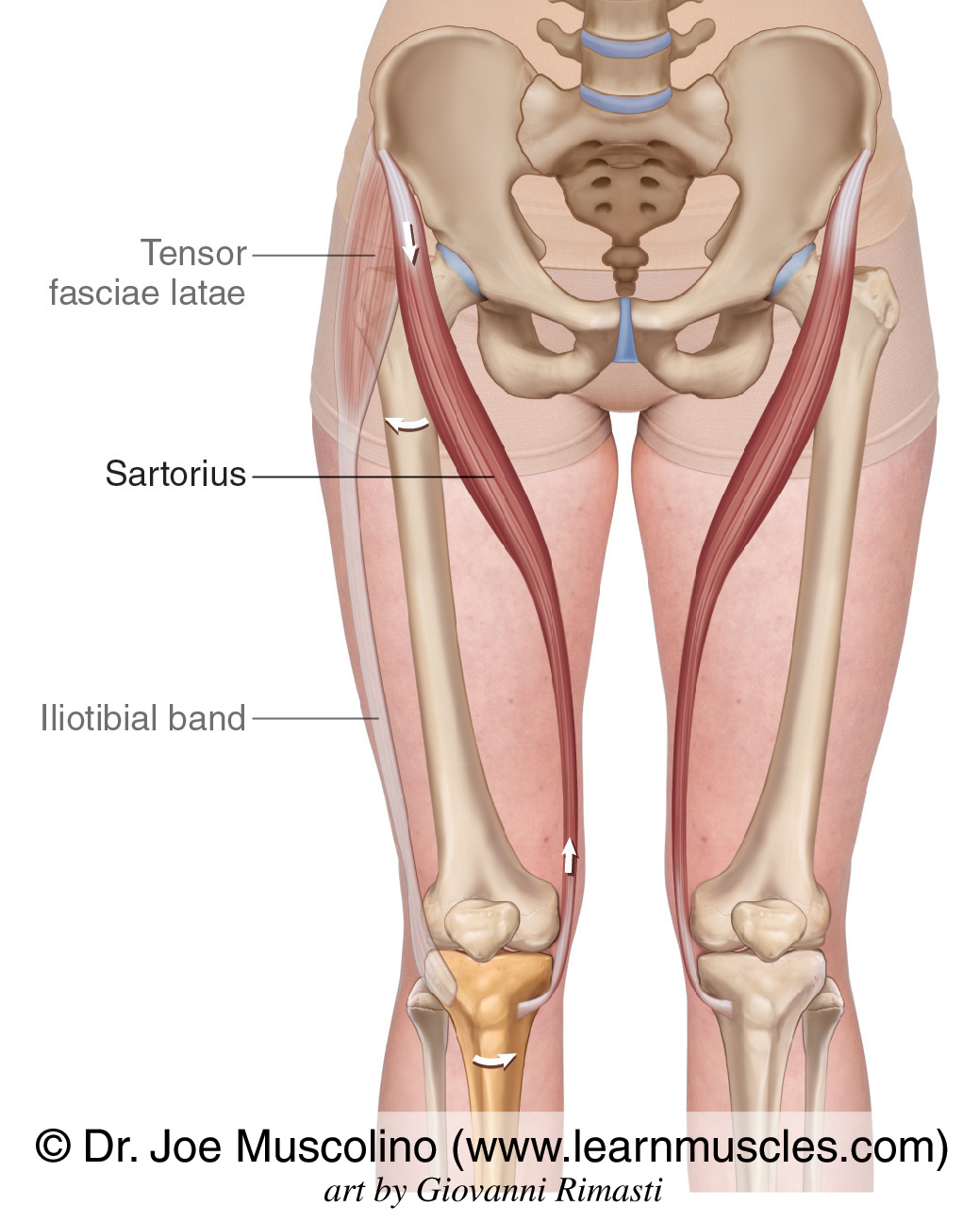
- Innervation: Femoral N.
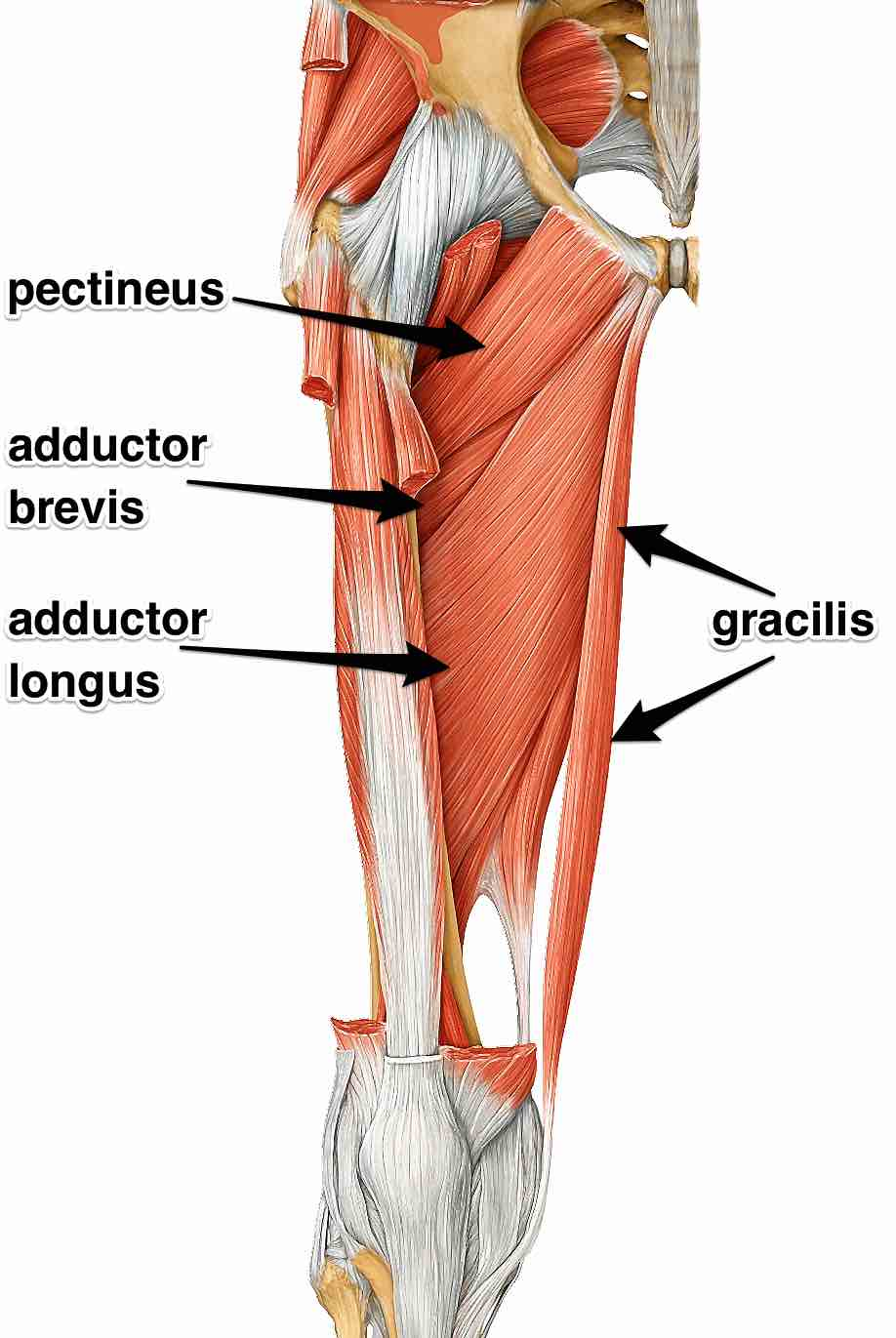
- Adductor Longus, Brevis, Magnus & Gracilis
- Action: Hip adduction.
- Innervation: Obturator N. (L2-L4).
- Clinical: Injury (e.g., pelvic surgery, fetal head compression) presents as gait instability and lateral swinging of leg.
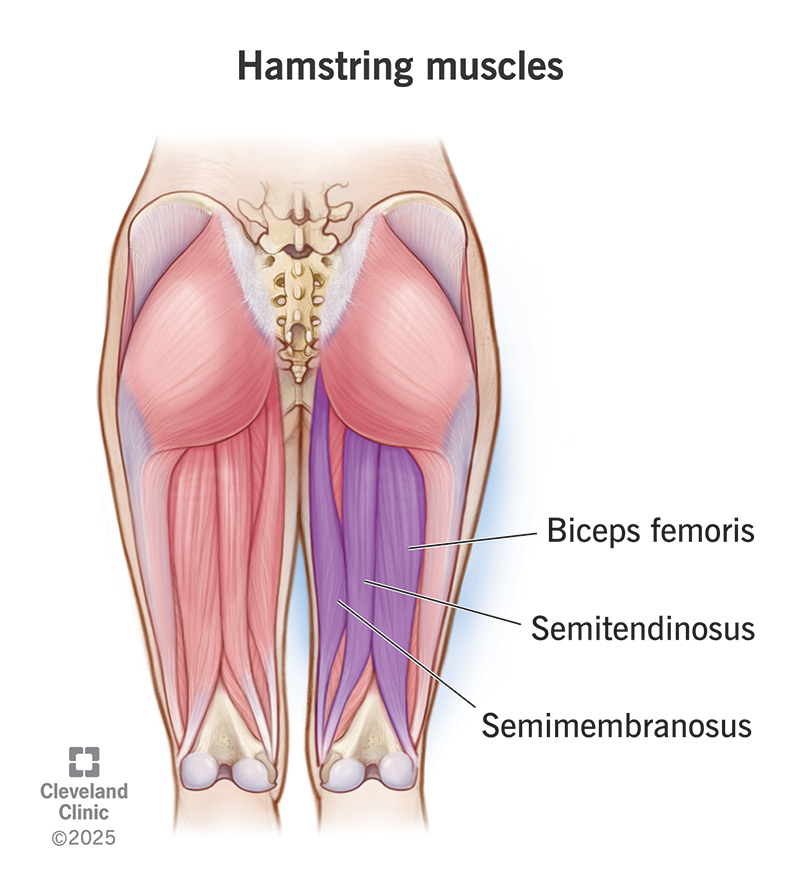
Thigh: Posterior Compartment (Hamstrings)
- Biceps Femoris, Semitendinosus, Semimembranosus
- Action: Hip extension, Knee flexion.
- Innervation: Sciatic N. (Tibial division; Short head of Biceps is Common Peroneal div).
- Clinical: Origin is the Ischial Tuberosity (avulsion fractures common in sprinters/hurdlers).
Leg: Anterior Compartment (Dorsiflexors)
- Tibialis Anterior
- Action: Dorsiflexion and Inversion.
- Innervation: Deep Peroneal (Fibular) N.
- Clinical:
- Nerve compression/trauma (fibula neck fracture affects common peroneal) → Foot Drop.
- Gait: Steppage gait (patient lifts leg high to clear toes).
- Extensor Hallucis Longus (EHL)
- Action: Big toe extension.
- Clinical: Used to test L5 nerve root motor function.
Leg: Lateral Compartment (Evertors)
- Peroneus (Fibularis) Longus & Brevis
- Action: Eversion and Plantarflexion.
- Innervation: Superficial Peroneal (Fibular) N.
- Clinical: Loss of sensation over dorsum of foot (spares webspace between 1st/2nd toes).
Leg: Posterior Compartment (Plantarflexors)
- Gastrocnemius & Soleus (Triceps Surae)
- Action: Plantarflexion.
- Innervation: Tibial N. (S1-S2).
- Clinical: Achilles Reflex (S1). Rupture feels like being “kicked in the back of the leg” + inability to tiptoe.
- Tibialis Posterior
- Action: Inversion and Plantarflexion.
- Innervation: Tibial N.
- Popliteus
- Action: Unlocks the knee joint (laterally rotates femur on fixed tibia) to initiate flexion.