- Pathophysiology/Etiology
- An imbalance between the amount of air reaching the alveoli (Ventilation) and the amount of blood perfusing them (Q).
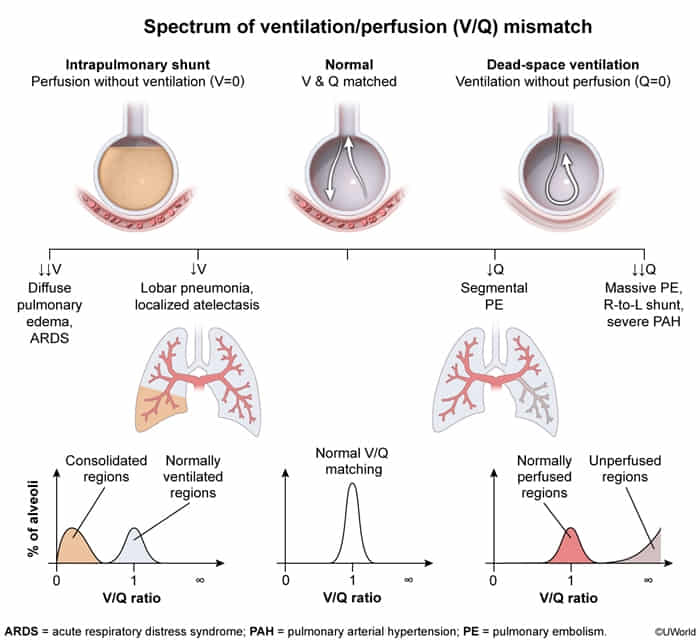
- The ideal V/Q ratio is ~0.8 to 1.0. Any significant deviation impairs gas exchange, leading to hypoxemia.
- An elevated A-a gradient is a hallmark of V/Q mismatch.
- Two Extremes of V/Q Mismatch
- 1. Low V/Q (Shunt): Perfusion without Ventilation (V/Q → 0)
- Mechanism: Blood flows past alveoli that are not ventilated (e.g., collapsed or filled with fluid), so it cannot be oxygenated. This is called a physiologic shunt.
- Causes: Airway obstruction (e.g., foreign body, mucus plug), pneumonia, pulmonary edema, atelectasis (lung collapse), ARDS.
- Key Feature: Hypoxemia that does not correct with 100% O2 because the supplemental O2 cannot reach the perfused capillaries.
- In a healthy, ventilated alveolus, hemoglobin passing by is already ~97-98% saturated with oxygen even on room air (21% O2).
- Only part of the blood redirect to healthy lungs, thus 100% O2 can’t entirely fix.
- 2. High V/Q (Dead Space): Ventilation without Perfusion (V/Q → ∞)
- Mechanism: Alveoli are ventilated, but there is no blood flow to them for gas exchange to occur. This is called alveolar dead space.
- Causes: Pulmonary embolism (PE) is the classic cause. Others include emphysema (capillary destruction), and conditions with low cardiac output or pulmonary hypertension.
- Key Feature: Primarily impairs CO2 elimination, leading to “wasted ventilation.” Hypoxemia occurs and typically corrects with 100% O2.
- Because all obstructed blood redirect to healthy arteries.
| Feature | Physiologic Shunt | Physiologic Dead Space |
|---|
| V/Q Ratio | Low (V/Q → 0) | High (V/Q → ∞) |
| Problem | No Ventilation (V) | No Perfusion (Q) |
| Pathophysiology | Airway obstruction, fluid-filled alveoli | Vascular obstruction, capillary destruction |
| Effect on Gas | Hypoxemia | Impaired CO2 removal, Hypoxemia |
| Response to 100% O2 | Does NOT Correct | Corrects |
| Classic Cause | Pneumonia, Pulmonary Edema | Pulmonary Embolism (PE) |
- Clinical Presentation
- Hypoxemia is the primary consequence.
- Symptoms depend on the underlying cause but can include dyspnea, tachypnea, dizziness, and cyanosis.
- Diagnosis
- Arterial Blood Gas (ABG): Shows hypoxemia (↓ PaO2).
- A-a Gradient: Increased A-a gradient is a key finding in V/Q mismatch, distinguishing it from hypoxemia due to hypoventilation or low inspired O2 (which have a normal A-a gradient).
- V/Q Scan: A nuclear medicine scan that directly measures and compares the distribution of ventilation and perfusion in the lungs. Classically used to diagnose PE.
- Imaging (CXR, CT): Helps identify the underlying cause (e.g., pneumonia, edema, PE).
- Management/Treatment
- Treat the underlying cause: This is the most crucial step (e.g., antibiotics for pneumonia, anticoagulation for PE, bronchodilators for asthma).
- Supplemental O2: Effective for high V/Q dead space but poorly effective for low V/Q shunts.
- Mechanical Ventilation: May be required for severe respiratory distress, often with PEEP to recruit collapsed alveoli in cases of shunting (e.g., ARDS).
- Key Differentiating Factors (High-Yield)
- Hypoxemia Correction with 100% O2:
- Corrects: Dead Space (e.g., PE).
- Does NOT correct: Shunt (e.g., pneumonia, pulmonary edema).
- A-a Gradient:
- Increased: V/Q Mismatch, Shunt, Diffusion limitation.
- Normal: Hypoventilation, High Altitude.