| Feature | Obstructive Pattern | Restrictive Pattern |
|---|---|---|
| Pathophysiology | ↑ Airway resistance. Problem getting air OUT. | ↓ Lung compliance/expansion. Problem getting air IN. |
| Spirometry - FEV1 | ↓↓ | ↓ |
| Spirometry - FVC | ↓ or Normal | ↓↓ |
| FEV1/FVC Ratio | < 0.7 (Hallmark finding)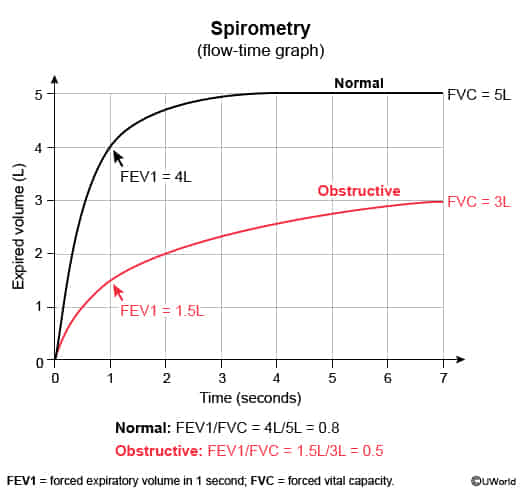 | > 0.7 (Normal or Increased)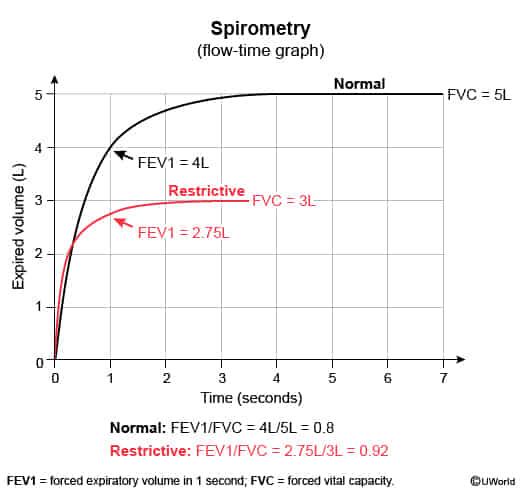 |
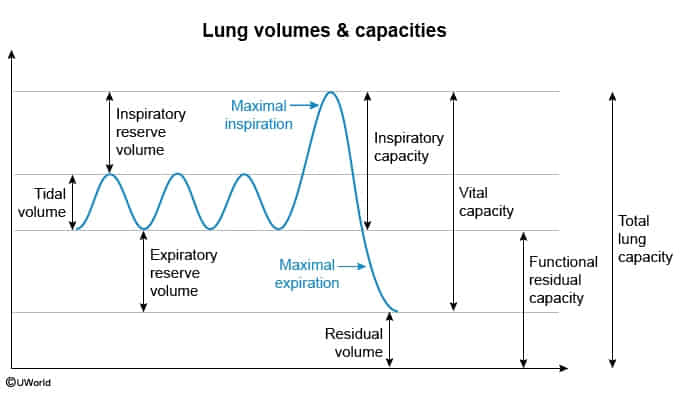
| Total Lung Capacity (TLC) | ↑ (due to air trapping) | ↓ (due to impaired filling) |
| Flow-Volume Loop | Concave, “scooped-out” expiratory limb | Shrunken loop, normal shape but smaller |
| Common Examples | COPD (Chronic Bronchitis, Emphysema) Asthma Bronchiectasis | Interstitial Lung Disease (e.g., IPF, Sarcoidosis) Chest Wall Disorders (Kyphoscoliosis, Obesity) Neuromuscular Disease (ALS, Guillain-Barré) |
| Clinical Findings | Wheezing, prolonged expiration, pursed lips, barrel chest (COPD) | Dyspnea on exertion, fine inspiratory (“Velcro”) crackles |
Obstructive Pattern
- Bronchiolitis obliterans
Restrictive Pattern
- Special case: Ankylosing spondylitis
- Pattern: Chest wall restriction from ankylosis/fusion of the costovertebral and costosternal joints → ↓ chest wall compliance, ↓ chest expansion, and ↓ vital capacity with a normal/↑ FEV1/FVC ratio.
- Why RV and FRC can be ↑: The rigid rib cage limits expiratory chest wall movement and fixes the thorax at a relatively expanded resting position. Because patients cannot fully deflate the lungs, residual volume (RV) increases; the higher end-expiratory volume also raises functional residual capacity (FRC). c
- Key idea: Restrictive physiology, but the problem is the chest wall cage rather than stiff lung parenchyma, so ↓ VC can coexist with ↑ RV/FRC.