Etiology
- Most common: Deep vein thrombosis
- Causes of nonthrombotic embolism
- Fat embolism
- Air embolism
- Amniotic fluid embolism
- Bacterial embolism
- Patients with intravenous drug use are at increased risk of developing tricuspid valve endocarditis, giving rise to septic pulmonary emboli
- Others: pulmonary tumor embolism, pulmonary cement embolism
Tip
Up to 30% of cases may present with no apparent risk factors (eg, hypercoagulability).
Pathophysiology
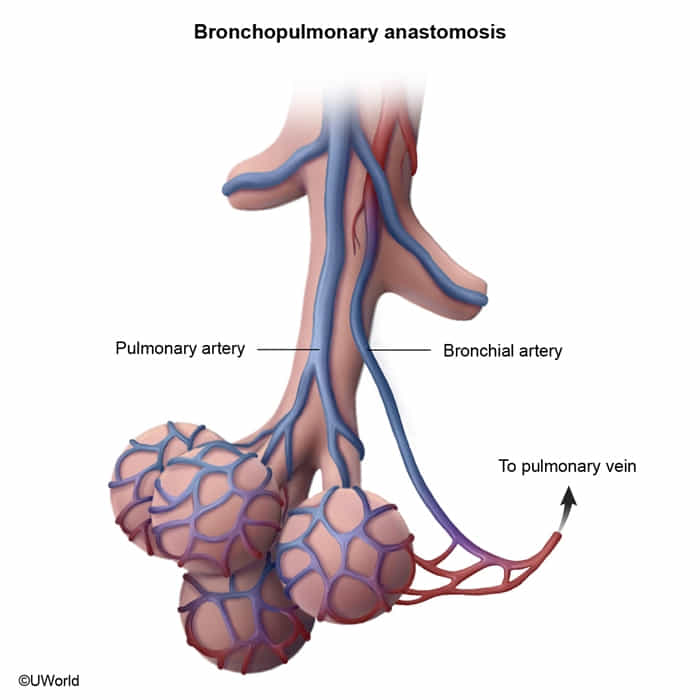
- Dual Blood Supply: The lungs are supplied by two circulations:
- Pulmonary Arteries: Low-pressure system carrying deoxygenated blood from the RV for gas exchange.
- Bronchial Arteries: High-pressure system arising from the aorta; supplies oxygenated blood to the lung parenchyma (bronchi, connective tissue).
- Pulmonary Infarction:
- Due to the dual blood supply, PE does not always cause pulmonary infarction (tissue death). The bronchial circulation can often sustain the lung tissue.
- Infarction is more likely to occur if the bronchial circulation is compromised (e.g., in left-sided heart failure) or if the embolus is very peripheral.
- When it occurs, it’s typically a hemorrhagic (red) infarct because some blood from the bronchial circulation still leaks into the necrotic area.
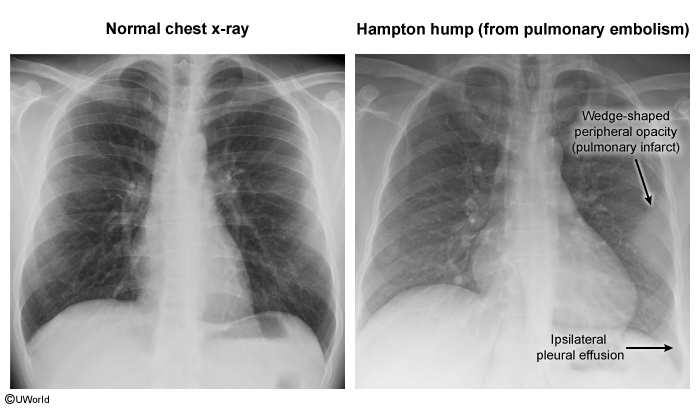
- Clinically, it presents with pleuritic chest pain and hemoptysis. Radiologically, it may appear as a wedge-shaped infiltrate (Hampton’s Hump).
Clinical features
- Common features of PE
- Acute onset of symptoms
- Dyspnea (> 75% of cases)
- Tachycardia and tachypnea (up to 50% of cases)
- Sudden pleuritic chest pain (∼ 20% of cases)
- Cough and hemoptysis
- Associated features of DVT: e.g., unilaterally painful leg swelling c
- Features of massive PE (e.g., due to a saddle thrombus)
- Presyncope or syncope
- Jugular venous distension and Kussmaul sign
- RV pressure overload
- Hypotension and obstructive shock
- Circulatory collapse
Diagnostics
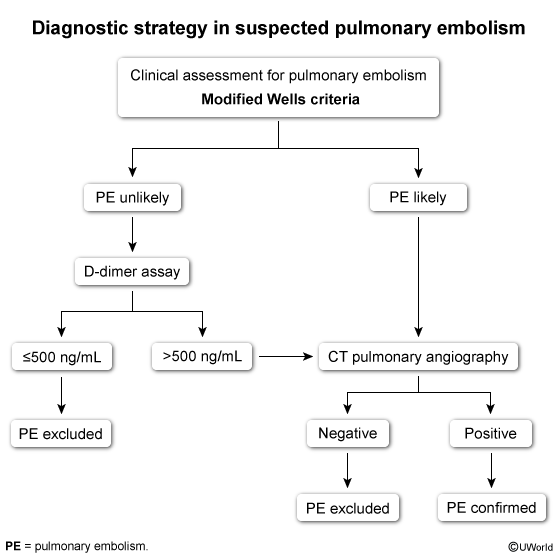
- Algorithm:
- Wells score (≤4 = PE unlikely; >4 = PE likely)
- +3 points
- Clinical signs of DVT
- Alternate diagnosis less likely than PE
- +1.5 points
- Previous PE or DVT
- Heart rate >100/min
- Recent surgery or immobilization
- +1 point
- Hemoptysis
- Cancer
- +3 points
- Hemodynamically Unstable: Bedside Echo → if RV strain → Treat.
- Stable + Low Prob (Wells ≤4): D-dimer (High sensitivity, low specificity). If (-) → Stop. If (+) → CTPA.
- Stable + High Prob (Wells >4): CTPA immediately. Start empiric anticoagulation before imaging if no contraindications.
- Wells score (≤4 = PE unlikely; >4 = PE likely)
- Initial/Adjuncts:
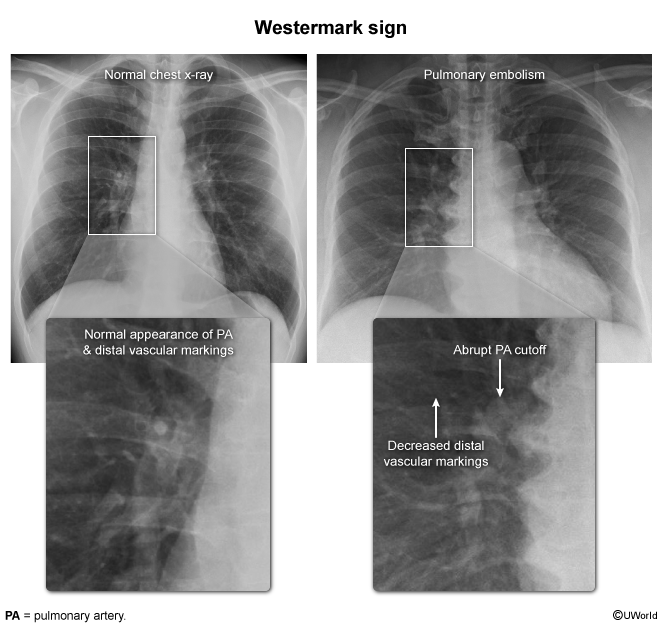
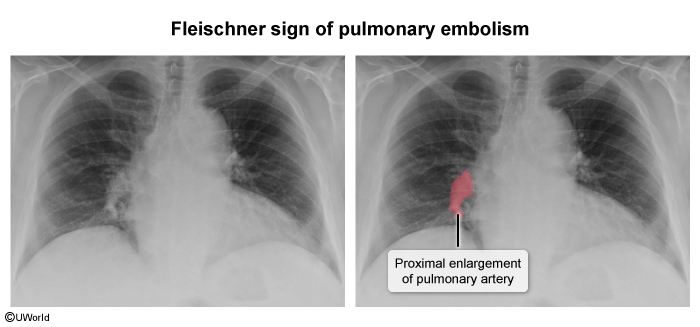
- CXR: Usually normal. Rare signs: Hampton Hump (wedge opacity), Westermark Sign (oligemia).
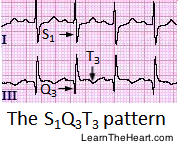
- ECG: Sinus tach (most common). S1Q3T3 (specific but rare, indicates RV strain).
- ABG: Respiratory alkalosis (hypocapnia), hypoxia, widened A-a gradient.
- CXR: Usually normal. Rare signs: Hampton Hump (wedge opacity), Westermark Sign (oligemia).
- Confirmatory/Gold Standard:
- CT Pulmonary Angiography (CTPA): Best initial test for most pts.
- V/Q Scan: Use if renal failure (Cr elevated), severe contrast allergy, or pregnancy (sometimes).
- Lower Extremity US: Useful if CTPA contraindicated/unavailable; (+) DVT treats as PE.
Treatment
Reperfusion therapy
- Indications
- Massive PE (hemodynamic instability and/or right heart failure) with a low bleeding risk
- Recombinant tissue plasminogen activator (tPA), e.g., alteplase (preferred)
- Endothelial-derived TPA is limited primarily to the bronchial circulation, and spontaneous recanalization of the pulmonary artery is a slow process.